
Uterine fibroids are benign tumors of the smooth muscles of the uterus. In some cases, there is abnormal uterine bleeding and pressure in the pelvis, occasionally also urinary or bowel problems, infertility or pregnancy complications. Diagnosis is made by gynecological examination, sonography and other imaging studies.
Uterine leiomyomas occur in around 40% of women of childbearing age. They are the most common benign tumors of the uterus. The different localizations of fibroids are listed in Overview 1.
Many uterine fibroids are asymptomatic (in 75% of patients) and are localized in the corpus uteri in over 90% of cases, the remainder in the cervix [1]. However, if women complain of symptoms such as dysmenorrhea or menorrhagia, a leiomyoma must be considered. Subserous fibroids, which account for 5 to 10% of all fibroids, are primarily responsible for bleeding, infertility and abortions. Large fibroids can lead to organ displacement and infertility is also possible. Sarcomatous degeneration is rare [2]. Lymphomas and metastases also lead to organ enlargement and are similar to fibroids [3]. An increase in size is not uncommon during pregnancy, and a reduction in size during the menopause.
Clinical examination with manual pelvic examination is the first diagnostic step, followed by transvaginal sonography. Symptomatic uterine fibroids are an indication for hysterectomy or arterial embolization.
Sonographically, clinically suspected uterine fibroids can be easily detected.
Further imaging is usually not necessary.
Exact preoperative localization can occasionally be difficult, and in the case of large or multiple fibroids, the ovaries and endometrium can also be assessed [4].
Subserosal localizations can also simulate solid ovarian tumors.
X-rays of the lumbar spine or pelvis occasionally reveal coarse intrapelvic structures that may indicate uterine fibroids.
Lymph node calcifications can also present a similar differential diagnosis.
Computed tomography scans show benign masses to be muscle-equivalent.
Due to oestrogen-stimulated growth, they can become definable in adulthood and show regressive changes in the menopause [2].
In the post-contrast scans, the image morphology is variable with hypodense, isodense or hyperdense imaging.
Large fibroids often show a heterogeneous structure after contrast administration.
Calcifications of the fibroids are present in over 10% of the growths and show a typical appearance.
After arterial embolization, cystic changes in the internal structure can be observed in addition to a reduction in size.
On magnetic resonance imaging, leiomyomas can be delineated as sharply defined nodular structures with hypointense signal in T1w and T2w sequences [4]. A pseudocapsule can often be differentiated. MRI is generally the method of choice in further diagnostic imaging procedures [5]. The indications are listed in Overview 2 .
Magnetic resonance imaging can differentiate between non-degenerative fibroids and degenerative fibroids, which show a heterogeneous signal. Endometrial carcinomas or sarcomas must then be differentiated. Small non-degenerated fibroids can hardly be distinguished from the muscularis, larger ones cause nodular contour changes and organ enlargement.
Case studies
In case example 1 (Fig. 1), a coarsely calcified fibroid of the uterus is visible as an incidental finding on an X-ray examination of the lumbar spine of a 77-year-old female patient. These coarse tuberous calcifications of varying sizes are typical of degenerated fibroids on X-ray.

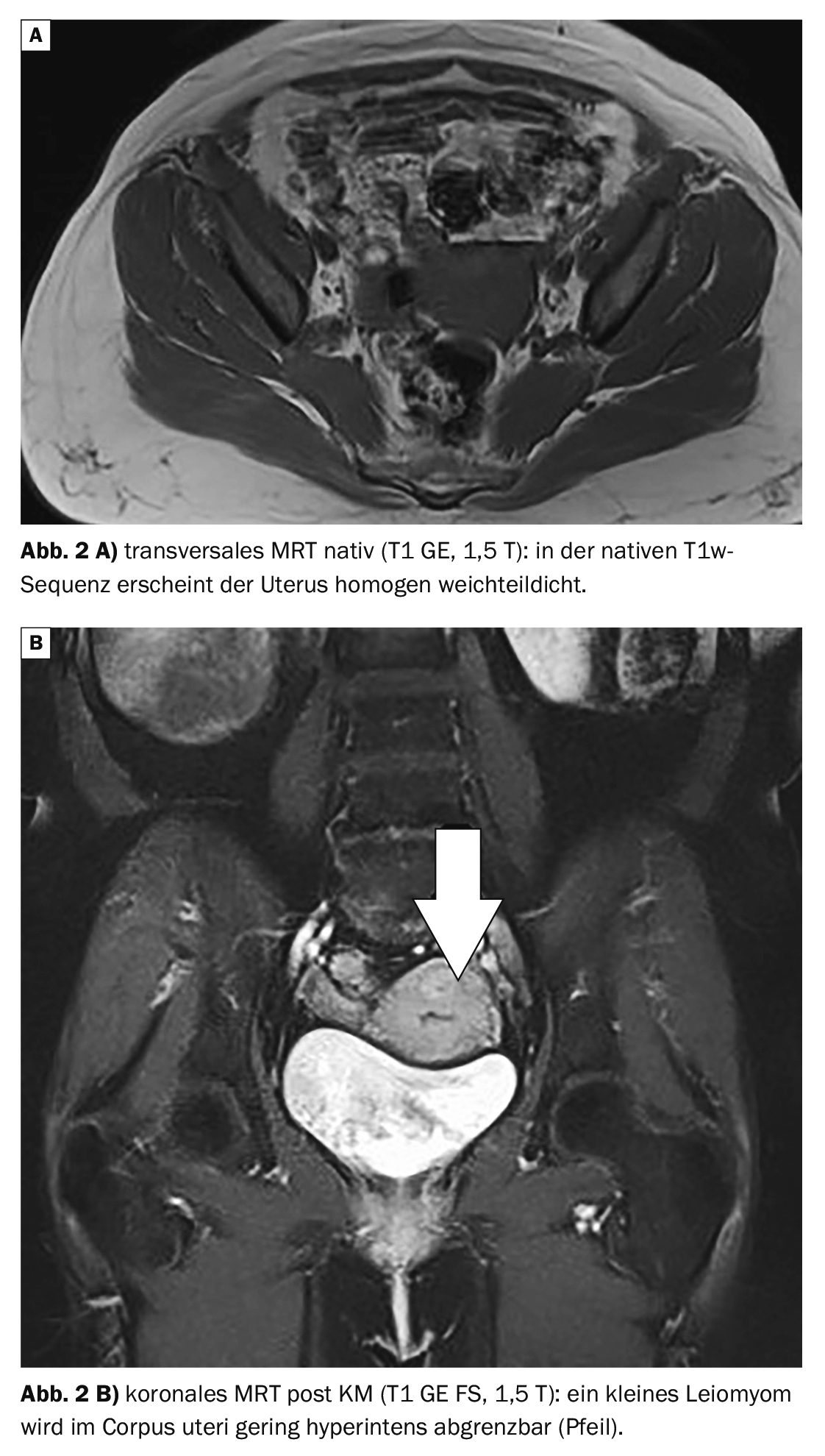
Case 2 demonstrates (Fig. 2A and 2B) a sinistropositioned uterus with several small fibroids up to 1 cm in an MRI of the pelvis. The 52-year-old patient complained of recurrent suprasymphatic pain.
Case 3 shows a 60-year-old female patient with a significantly enlarged uterus with several fibroids up to 4.6 cm in diameter (Fig. 3A and 3B). This resulted in an impression of the bladder roof with dysuria.

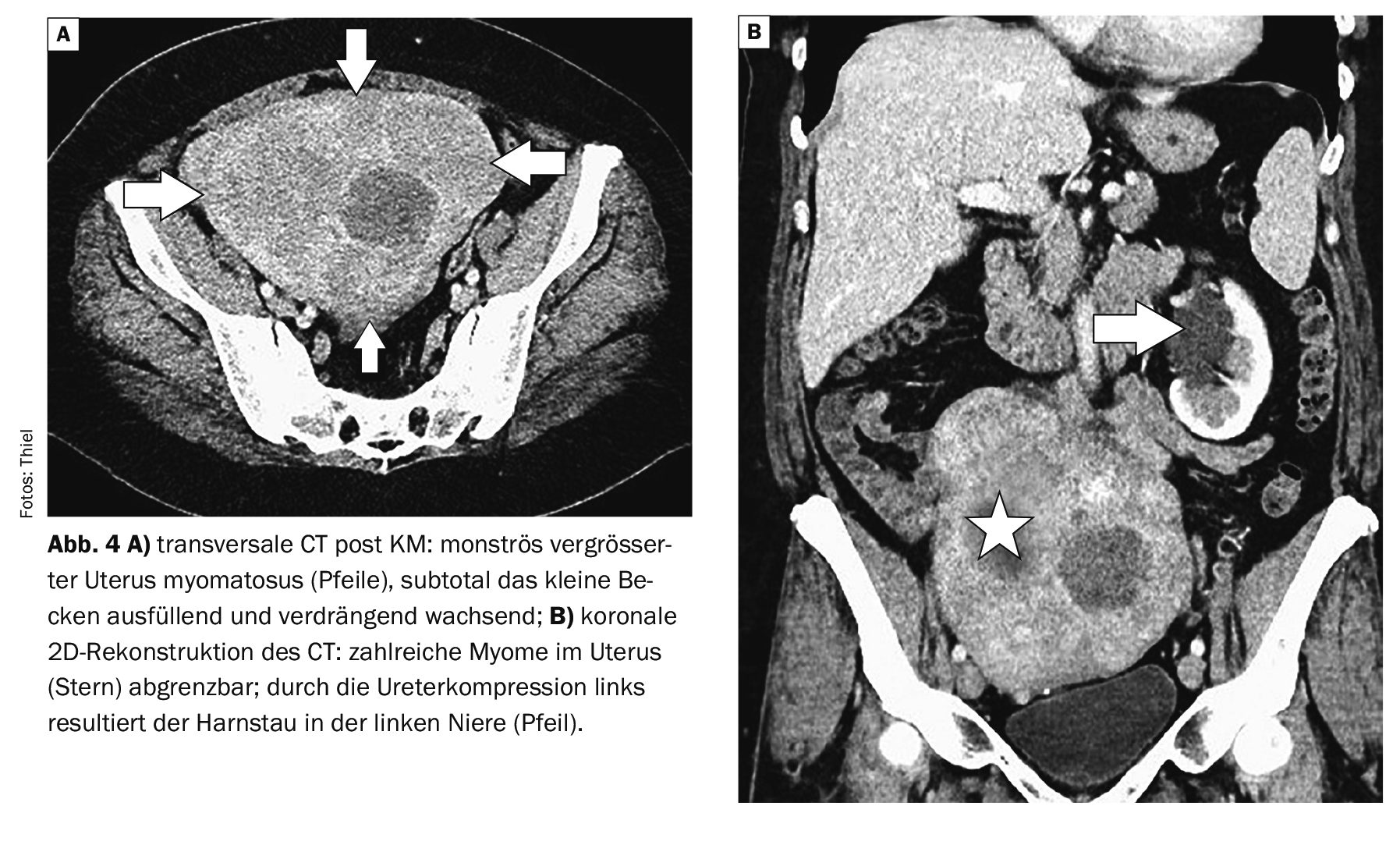
Case study 4shows a uterus myomatosus with a diameter of more than 16 cm in computed tomography images. This resulted in a clear displacement of the adjacent organs. The stenosis of the left ureter led to a congestion of the hollow system of the left kidney and considerable compression of the urinary bladder (Fig. 4A and 4B).
Take-Home-Messages
- Leiomyomas of the uterus are primarily benign masses that rarely degenerate into sarcomas.
- They have different localizations in the uterus.
- They are usually clinically silent, but can also be accompanied by considerable symptoms, primarily dysmenorrhea, menorrhagia and, depending on their size, infertility and abortions.
- In addition to manual gynecological examinations and transvaginal ultrasound, magnetic resonance imaging plays an important role in imaging.
- Therapeutically, arterial embolization and hysterectomy are indicated for treatment-resistant symptoms.
Literature:
- Rummeny EJ, Reimer P, Heindel W (eds.): Whole-body MR tomography. Georg Thieme Verlag Stuttgart, New York 2002; pp. 414.
- Prokop M, Galanski M; Co-Editors: van der Molen A, Schaefer-Prokop CM. Computed Tomography of the Body. Georg Thieme Verlag Stuttgart, New York 2003; pp. 712.
- Burgener FA, et al: Differential diagnostics in MRI. Georg Thieme Verlag Stuttgart, New York: 2002; pp. 620.
- Keller M, Kubik-Huch RA: Importance of cross-sectional imaging in the diagnosis of diseases of the female genital tract. Radiology up2date 2001; 3: 235-255.
- Alt CD, Kubik-Huch RA: Diagnosis and staging of gynecological tumors using MRI. Radiology up2date 2017; 17: 183-197.
- Kamp D, van den Höfel N: Uterusmyom. flexikon.doccheck.com/en/Uterusmyom, (last accessed 02.07.2024).







