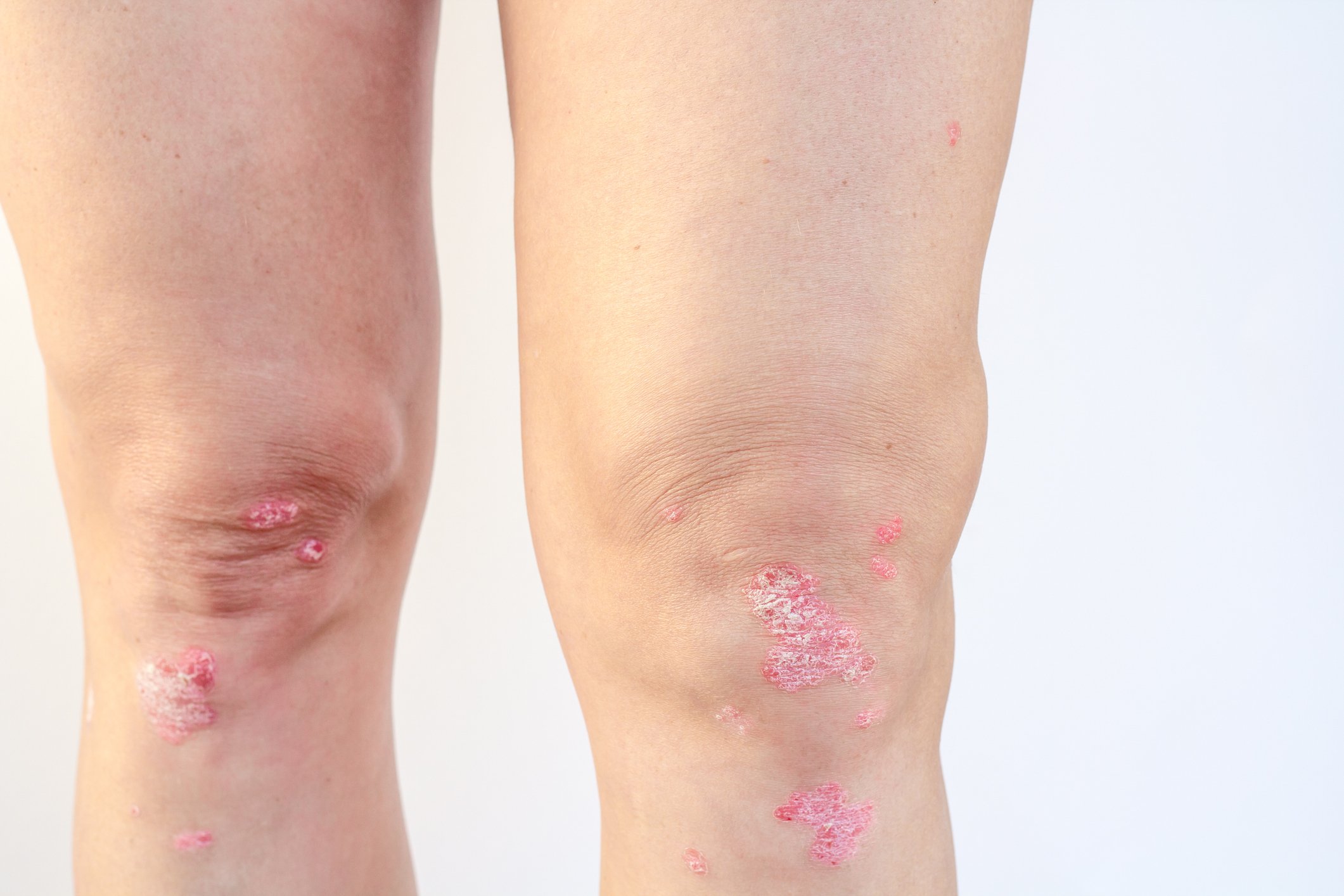
Psoriatic arthritis (PsA) affects about one in three patients with psoriasis and, if left untreated, can lead to severe physical limitations and a reduced quality of life [2,3]. With the newly obtained reimbursement of a biologic, adults with PsA can now benefit from a long-term effective treatment option with a stable safety profile and patient-friendly use [1,4,5].
Since March 2022, risankizumab (SKYRIZI®; 150 mg), nearly three years after its approval for moderate-to-severe plaque psoriasis, can also be used as monotherapy or in combination with conventional systemic disease-modifying antirheumatic drugs (csDMARDs) for the treatment of adults with active PsA who have had an inadequate response to or have been intolerant of one or more csDMARDs [4, 6, 7]. The cost of this treatment has been covered by health insurance since September 2022, although the prescription can only be made by specialists in dermatology or rheumatology or dermatological or rheumatological university hospitals/polyclinics [1]. In addition to the Janus kinase (JAK) inhibitor upadacitinib (RINVOQ®), AbbVie offers risankizumab as another valuable therapeutic option in PsA [4, 8].
One of the features of the selective IL-23 inhibitor is a patient-friendly 3-month treatment interval after 2 initial injections at weeks 0 and 4 [4, 5]. The dosage and the administration interval are thus the same in both indications psoriasis and PsA [4]. The long-term efficacy of risankizumab and its beneficial and stable safety profile in psoriasis and PsA have been demonstrated in several phase III studies [5, 9-12]. That risankizumab positively affects disease progression in patients with active PsA is shown by the results of the randomized, placebo-controlled, phase III KEEPsAKE 1 and 2 trials [3, 13].
Proven efficacy and good tolerability in PsA. [3, 13]
In KEEPsAKE 1 and 2, a total of 1408 adult PsA patients with inadequate response or intolerance to conventional synthetic (cs) DMARDs (KEEPsAKE 1) and/or biological (b) DMARDs (KEEPsAKE 2) randomized to 24 weeks of double-blind treatment with risankizumab (150 mg) or placebo. In the subsequent open-label extension (OLE), all patients received risankizumab. After 24 weeks, significantly more patients achieved the primary endpoint of a 20% response to the various American College of Rheumatology criteria (ACR 20) with risankizumab than with placebo in both studies(Table). Significantly better results were also obtained in the risankizumab arm in terms of 50% ACR 50 and 70% ACR 70 response, as well as improvement in enthesitis, dactylitis, fatigue, and physical functionality [3, 13]. According to recent data presented at the 2021 EADV Congress, the efficacy of risankizumab in OLE continued to increase numerically. For example, the ACR 20 response rate in patients continuously treated with risankizumab at 52 weeks was 70.0% in KEEPsAKE 1 and 58.5% in KEEPsAKE 2, which included patients with inadequate response to previous bDMARDs [12]. Overall, risankizumab was well tolerated and the safety profile was comparable to that observed in patients with psoriasis [3, 13].

Table: Response of patients with active psoriatic arthritis under RISA after 24 weeks in the PBO-controlled, randomized phase III studies KEEPsAKE 1 and 2.
Patients in KEEPsAKE 1 had previously responded inadequately to or failed to tolerate ≥ 1 csDMARDs. Patients in KEEPsAKE 2 had previously responded inadequately to or failed to tolerate ≤ 2 bDMARDs and/or ≥ 1 csDMARD.
Non-responder imputation (NRI) with multiple imputations if data are missing due to COVID-19, or NRI if no data are missing due to COVID-19. *p<0.05; **p<0.01; ***p< 0.001
◾ Defined as Leeds Enthesitis Index (LEI)=0 in patients with LEI>0 at baseline.
◽ Defined as Leeds Dactylitis Index (LDI)=0 in patients with LDI>0 at baseline.
RISA: 150 mg risankizumab at weeks 0, 4, and 16; PBO: placebo; ACR 20/50/70: improvement in American College of Rheumatologycriteria by 20/50/70%; HAQ-DI: Health Assessment Questionnaire-Disability Index; FACIT-Fatigue: Functional Assessment of Chronic Illness Therapy-.
Fatigue Questionnaire. Adapted from [3, 13]
Conclusion
As shown by the results of KEEPsAKE 1 and 2, treatment with risankizumab can significantly alleviate PsA-associated symptoms and achieves similar efficacy in PsA as existing treatment options [3, 13]. In addition, risankizumab showed the highest efficacy in moderate to severe plaque psoriasis in head-to-head studies compared with ustekinumab, secukinumab, and adalimumab [5, 10, 11]. With the reimbursement of the selective IL-23 inhibitor risankizumab, adult patients with active PsA can benefit from a long-term effective treatment option with a stable safety profile and patient-friendly use [1, 4, 5].
Literature
- Federal Office of Public Health Specialty List. www.spezialitaetenliste.ch.
- Rheumatism League Switzerland. Psoriatic Arthritis Patient Brochure. https://www.rheumaliga.ch/assets/doc/ZH_Dokumente/Broschueren-Merkblaetter/Krankheitsbilder/Psoriasis.pdf.
- Ostor A et al. Efficacy and safety of risankizumab for active psoriatic arthritis: 24-week results from the randomised, double-blind, phase 3 KEEPsAKE 2 trial. Ann Rheum Dis, 2022. 81(3): p. 351-358.
- Current SKYRIZI® (risankizumab) technical information at www.swissmedicinfo.ch.
- Gordon KB et al. Efficacy and safety of risankizumab in moderate-to-severe plaque psoriasis (UltIMMa-1 and UltIMMa-2): results from two double-blind, randomised, placebo-controlled and ustekinumab-controlled phase 3 trials. Lancet, 2018. 392(10148): p. 650-661.
- Swissmedicjournal 04/2019. Viewable at https://www.swissmedic.ch/swissmedic/de/home/ueber-uns/publikationen/swissmedic-journal/swissmedic-journal-2019.html.
- Swissmedicjournal 03/2022. Viewable at https://www.swissmedic.ch/swissmedic/de/home/ueber-uns/publikationen/swissmedic-journal/swissmedic-journal-2022.html.
- Current technical information RINVOQ® (upadacitinib) on www.swissmedicinfo.ch
- Papp KA et al. Long-Term Efficacy and Safety of Risankizumab for the Treatment of Moderate-to-Severe Plaque Psoriasis: Interim Analysis of the LIMMitless Open-Label Extension Trial Beyond 3.5 Years of Follow-Up. P1354, presented at the30th EADV Congress Sept. 29-Oct. 02, 2021.
- Warren RB et al. Efficacy and safety of risankizumab vs secukinumab in patients with moderate-to-severe plaque psoriasis (IMMerge): results from a phase III, randomized, open-label, efficacy-assessor-blinded clinical trial. Br J Dermatol, 2021. 184(1): p. 50-59.
- Reich K et al. Risankizumab compared with adalimumab in patients with moderate-to-severe plaque psoriasis (IMMvent): a randomised, double-blind, active-comparator-controlled phase 3 trial. Lancet, 2019. 394(10198): p. 576-586.
- Kristensen LE et al. Efficacy and Safety of Risankizumab for Active Psoriatic Arthritis: 52-Week Results From the KEEPsAKE 1 and KEEPsAKE 2 Trials. D1T01.4A. Presented at30th EADV Virtual Congress 28.09.-02.10.2021.
- Kristensen LE et al. Efficacy and safety of risankizumab for active psoriatic arthritis: 24-week results from the randomised, double-blind, phase 3 KEEPsAKE 1 trial. Annals of the Rheumatic Diseases, 2022. 81(2): p. 225-231.
- McInnes IB et al. Trial of Upadacitinib and Adalimumab for Psoriatic Arthritis. N Engl J Med, 2021. 384(13): p. 1227-1239.
- Mease PJ et al. Upadacitinib for psoriatic arthritis refractory to biologics: SELECT-PsA 2. Ann Rheum Dis, 2021. 80(3): p. 312-320.
- McInnes IB et al. Upadacitinib in patients with psoriatic arthritis and an inadequate response to non-biological therapy: 56-week data from the phase 3 SELECT-PsA 1 study. RMD Open, 2021. 7(3).
The references can be requested by professionals at medinfo.ch@abbvie.com.
To the brief technical information of SKYRIZI® and RINVOQ®.
With the financial support of AbbVie AG, Alte Steinhauserstrasse 14, 6330 Cham.
Article online since 07/09/2022
CH-SKZR-220003_08/2022