
The diagnosis of ADHD (attention deficit hyperactivity disorder) seems to be on the rise and appears remarkably frequently in TV documentaries and audio podcasts. However, it remains unclear whether ADHD is really more common than the usual 5-8% prevalence in children due to our fast-moving times with multitasking and high performance demands, or whether more people are now being diagnosed who previously had other diagnoses or fell through the cracks. The adult prevalence is around 6%, whereby approx. 87% of those diagnosed in adulthood had no diagnosis in childhood!
The diagnosis of ADHD (attention deficit hyperactivity disorder) seems to be increasing at an explosive rate and appears remarkably frequently in TV documentaries and audio podcasts. However, it remains unclear whether ADHD really occurs more frequently than the 5-8% prevalence of children usually quoted [1] due to our fast-moving times with multitasking and high performance demands, or whether more people are now being diagnosed who previously had other diagnoses or fell through the cracks. Because most symptoms of inattention persist into adulthood, the adult prevalence is around 6% [2], although in an Australian study [3] 87% of those diagnosed in adulthood had no diagnosis in childhood!
You can take the CME test on our learning platform after you have reviewed the recommended materials. Please click on the following button:
In any case, people with ADHD keep us busy more often in GP surgeries: on the one hand, ADHD sufferers end up with us because there are no more psychiatrists available to continue their medication. On the other hand, they are “annoying” patients who forget their appointments, pay their bills too late or, due to their restlessness, upset our consultation hours first and then the receptionist at the end.
This article – based on a presentation at the SGAIM Autumn Congress 2024 – is intended to provide primary care providers with basic knowledge on diagnostics and treatment in order to provide effective relief for these people, who often suffer very severely.
Symptoms
The classic ADHD symptoms can be found in Table 1; however, in addition to the diagnosis-defining symptoms, those in the bottom section are also clinically significant.
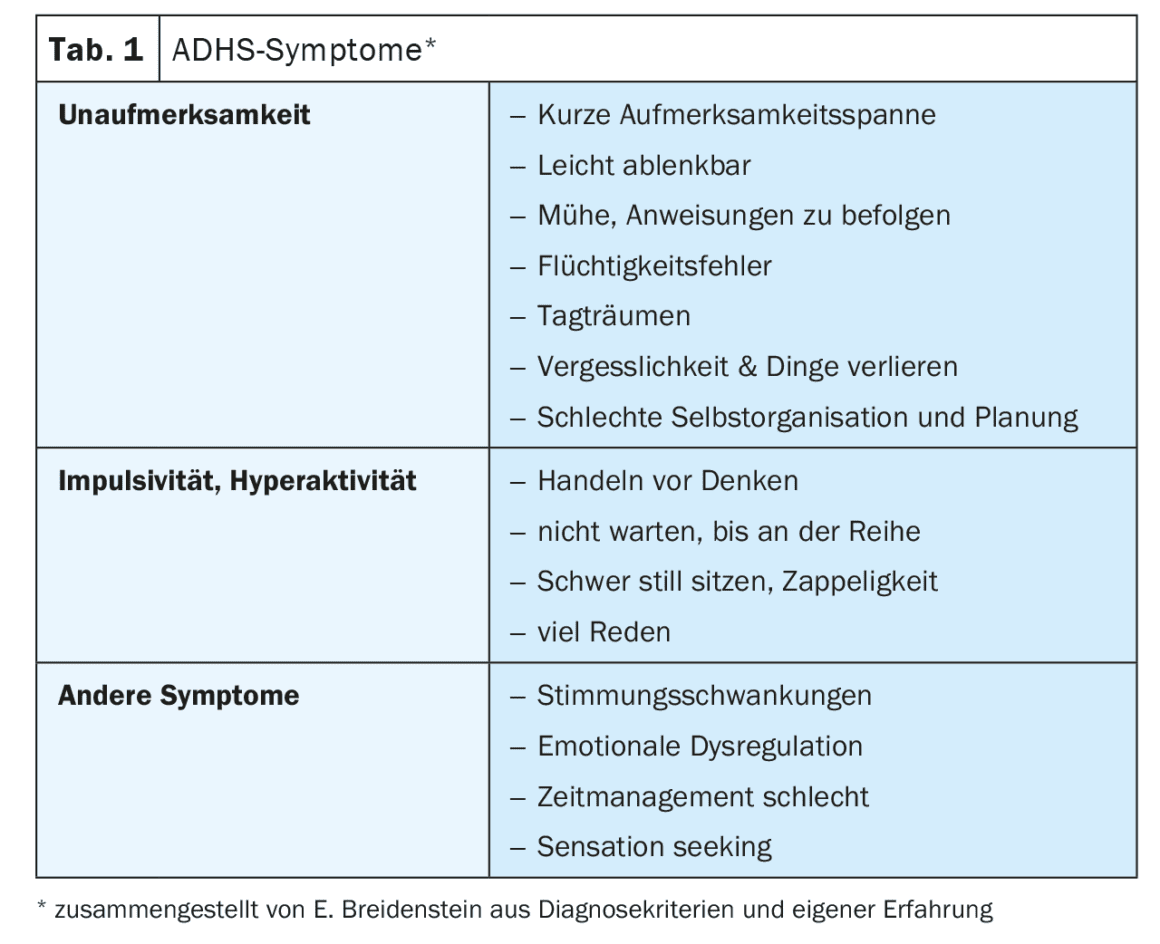
All of the behaviors mentioned in the introduction are symptoms of ADHD; the patients don’t do it to annoy us, but because they can’t help it. They are also ashamed of this – and their self-esteem suffers. However, previously undetected ADHD could also be behind exhaustion depression in women in their 30s, men with “dishwasher careers” and burnout, addictions or repeated accidents (from minor accidents to speeding accidents in traffic or on skis); the crises mentioned occur because previous compensation strategies or self-medication attempts fail.
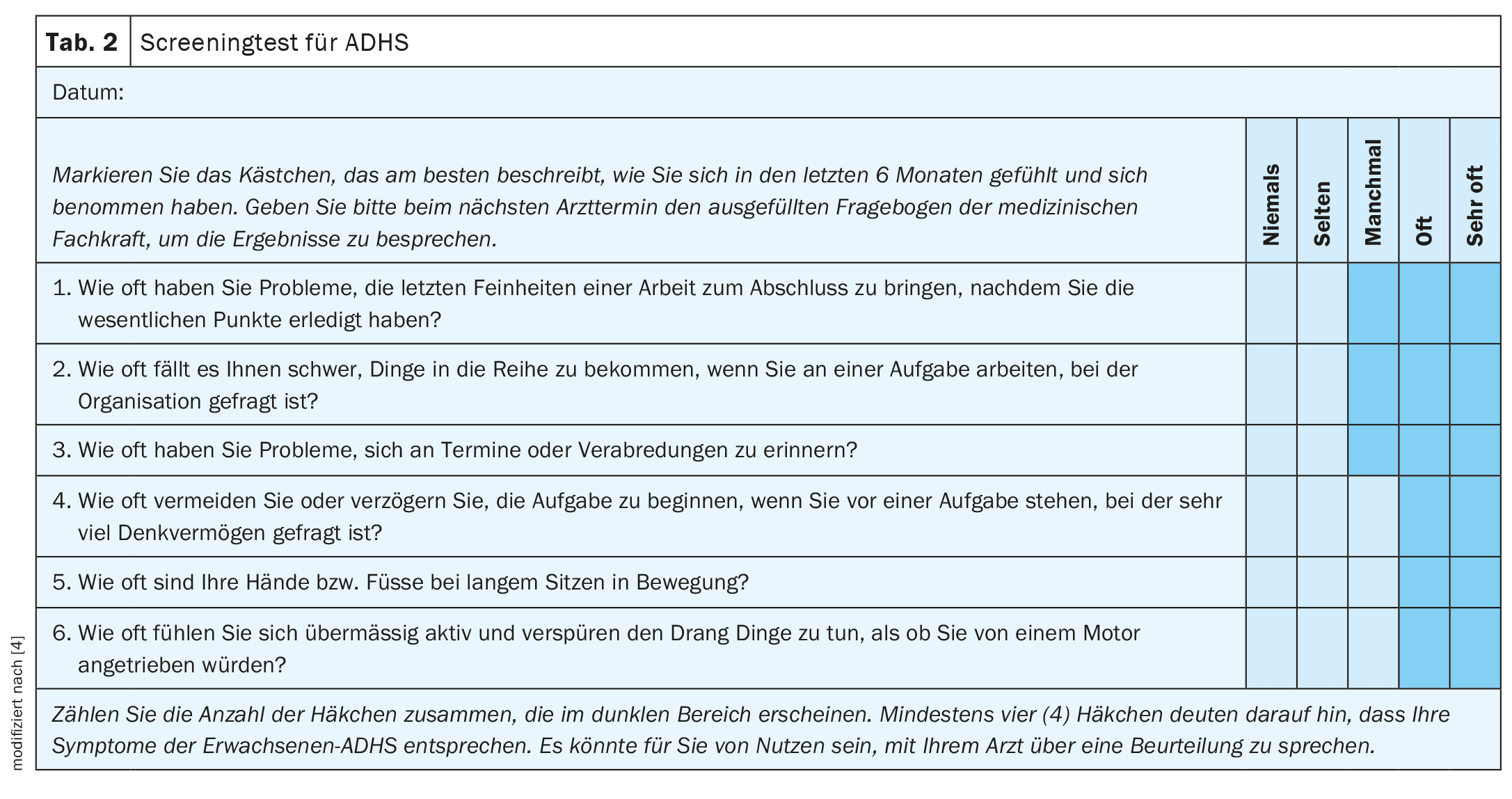
If ADHD is suspected, it is worth carrying out the WHO screening questionnaire (ASRS-V1.1, Tab. 2 [4]) and, if necessary, seek clarification from a psychiatrist or psychologist.
Comorbidities with ADHD
Psychologists can also make the diagnosis, can be useful for everyday coping and are particularly important in the case of comorbidities. This is because over 50% of people diagnosed with ADHD since early childhood have a psychiatric comorbidity in adulthood [5]:
- Partial performance disorders (perceptual and motor disorders, dyslexia, etc.)
- Depression, bipolar disorders; anxiety, compulsions
- Sleep disorders
- Substance abuse, addiction
- Personality disorders, schizophrenia.
There is also a large overlap (40-50%) with autism spectrum disorder and sensory hypersensitivity; these combinations make life all the more stressful, so that states of exhaustion become more frequent.
But ADHD also has many somatic effects that we as primary care providers should be aware of and treat [6]: It doubles the risk of heart problems and CHD, nicotine abuse and sleep problems. Dental problems and an increase in BMI as well as teenage pregnancies and sexually transmitted diseases are also much more common than in the normal population.
Differential diagnostics
It is also important to rule out somatic differential diagnoses such as iron deficiency, which exacerbates the dopamine deficiency, sleep apnoea syndrome or hormone dysfunctions that can mimic ADHD symptoms (hyperparathyroidism, thyroid dysfunction or sex hormone deficiency). The menopause can unmask previously compensated ADHD because oestrogen influences the dopamine effect in the brain [7].
Pathophysiology of ADHD
ADHD is a multi-genetic neurodiversity with 60-80% inheritance. Interestingly, however, the phenotype is different in each generation, i.e. more or less hyperactive or more or less additional autism symptoms.
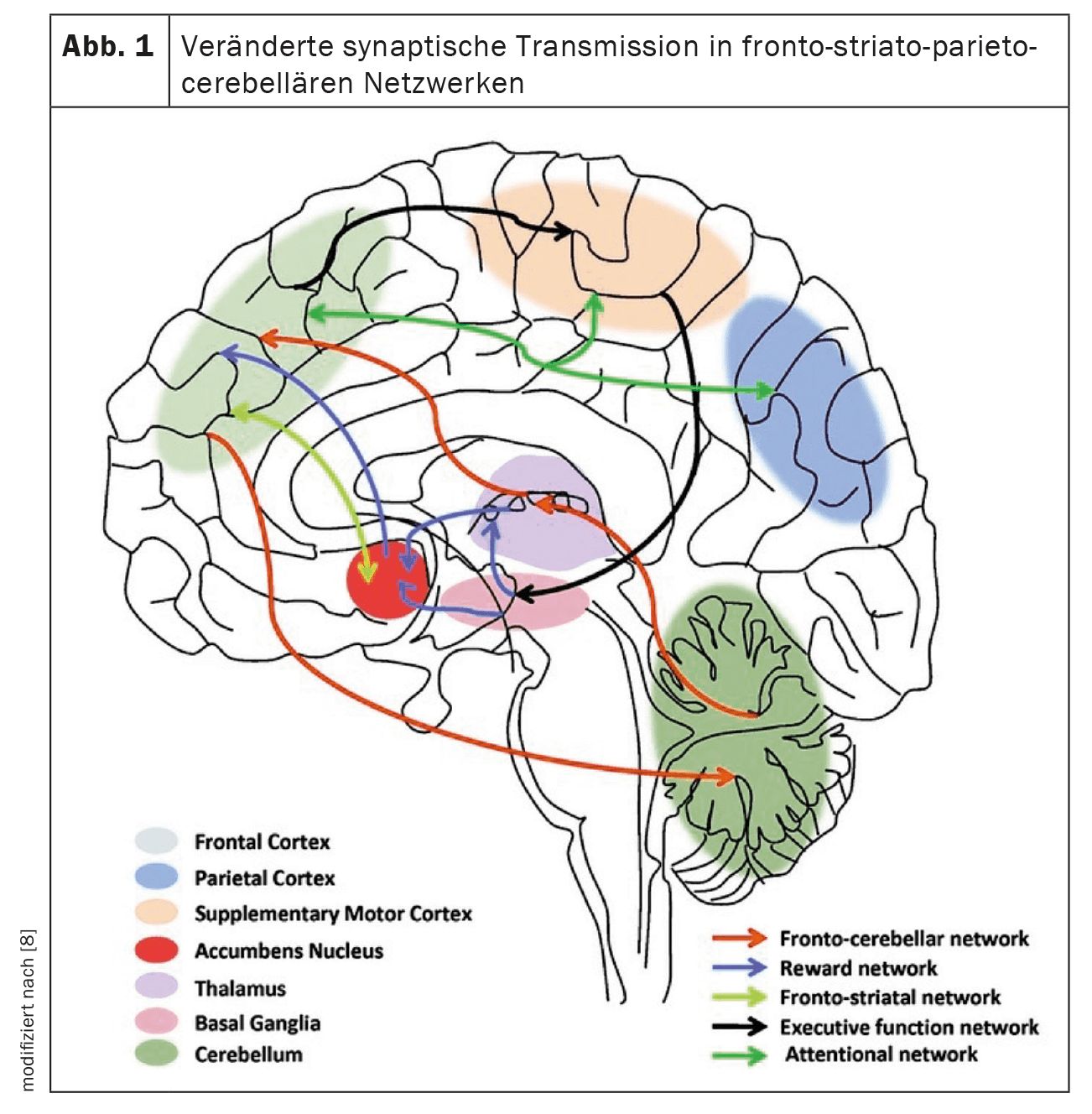
ADHD-associated mutations are shown for: Hypoactivity and dysregulation of dopamine, noradrenaline and in some cases serotonin (reduced synaptic transmission in certain networks in the brain) [8] with corresponding impairment of the executive functions localized there (Fig. 1):
- Fronto-parietal: attention, impulse-behavior and emotion control
- Fronto-striatal: attention, working memory, emotion control
- Mesocortico-limbic system: Maintaining motivation
- Fronto-cerebellar: motor impulse control & coordination.
Environmental factors such as peri- and postnatal brain damage, psychological adversities in childhood, chemical stress (e.g. chronic lead exposure) [9] or pathologies in the gut-brain axis or food intolerances also contribute to the penetrance of the genes [10].
The development of certain (e.g. inhibitory) brain areas can be delayed by up to four years in ADHD [11], which leads to discrepancies between biological and chronological performance
in everyday adolescent life – and demands a great deal of support from parents. Unfortunately, however, parents affected by ADHD also have poorer structuring skills and possibly a poorer socio-economic situation in the family, which can lead to a negative environment-genetics interaction.
Non-drug treatment
Recognize excessive demands on yourself (caution: dual role, helper syndrome,…)
People with ADHD tend to exceed their energy limits because they are so open to stimuli and see everything that is interesting and in need of help and have difficulty saying no; on the other hand, they also need more recovery time than other people. Primary care providers can set an important preventive or early “secondary prophylactic” course in terms of education, but also in very practical terms by providing relief for everyday life (e.g. Spitex, external childcare, “senior citizens’ network”).
Provide structures and use “pedagogical” means
Thanks to our long-standing relationships as general practitioners and family doctors, we can take advantage of the opportunity for a certain amount of “post-relief” and practise everyday skills with ADHD sufferers, the non-fulfilment of which in the “normal” world always ends in social disaster (from job loss to tax debts). This includes, for example:
- Help to keep appointments, use reminder functions in the cell phone and have them programmed during the appointment, possibly SMS reminder for the appointments by MPA
- Invoices: send reminders, call and arrange installment payments
- Design consultation structure dominated by the doctor (so that you don’t get lost and important things can also be discussed …)
- Obtain timely feedback (both on life changes and medication trials).
If this is not enough, support from occupational therapy and psychotherapy (via basic insurance) or ADHD coaching (self-pay) can help; the structuring skills mentioned above can be practiced intensively with these specialists. Address lists are available from the specialist association sfg-adhs.ch.
ADHD also has advantages
It would be a great shame if ADHD strengths were not able to enrich our society due to the aforementioned ADHD-related difficulties:
Because the “ADHD brain thinks differently”, new solutions are possible, creative other approaches can be combined with each other in the associatively networked brain; one ventures energetically and impulsively into completely new business ideas without having to budget long over advantages and disadvantages (why did the founder of Ikea make operating instructions possible without words or, for example, David Neeleman founded Jetblue and invented the e-ticket? [12]).
Many ADHD people have had to learn to pick themselves up and move forward due to numerous setbacks; they are well-trained “stand-up people”. Because procrastination is an all-too-common ADHD symptom, they have experience in improvising and purposefully moving forward under pressure; in fact, you could say that the ADHD brain runs at an ideal operating temperature with good levels of stress hormones. Perhaps this is why the ADHD rate in blue light jobs is so high.
Coupled with good specialist knowledge and the combination of high sensitivity and omnidirectional, i.e. undirected attention, ADHD people are often able to perform their role as supervisor more competently than others because they “see everything and feel everything”.
Once ADHD sufferers have found their dream job, they can block out everything disruptive in their hyperfocus and work forward with a high level of concentration or achieve top performance in the shortest possible time. Interestingly, this is often not perceived as anything special by those affected and they forget to give themselves the break they actually need after this performance.
ADHD medication
Individual choice of medication and dosage
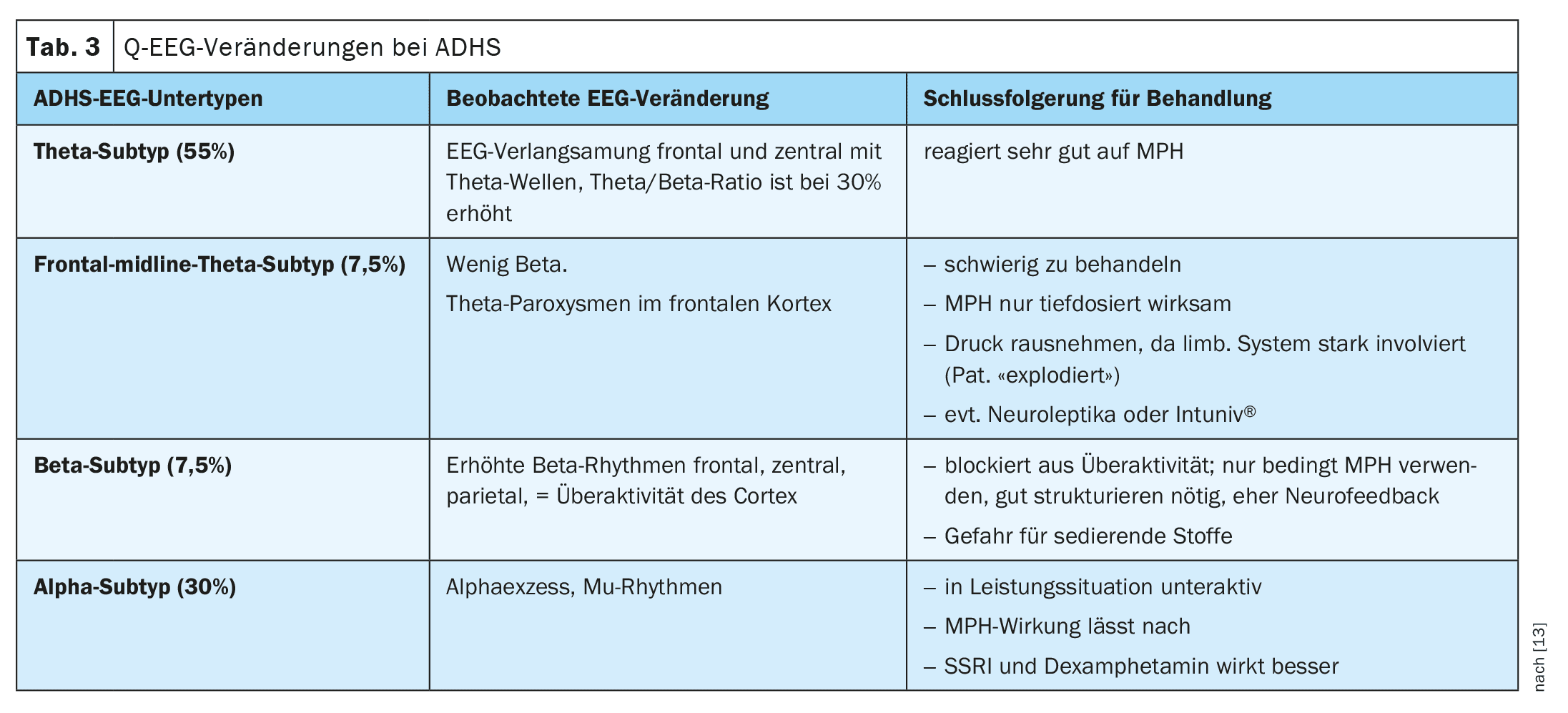
Because ADHD is diagnosed clinically, i.e. on the basis of the classic symptoms, different brain dysfunctions may be behind the same phenotypes. The activity of the different brain regions could be investigated using a complex quantitative EEG (qEEG) [13]. In the most common type of ADHD, the frontal brain produces theta waves, as in the sleep state; when these people are “woken up” with methylphenidate, both attention control and restlessness normalize. However, since there are also other qEEG types (which also show ADHD symptoms) that react poorly or very sensitively to methylphenidate, the medication must be titrated very carefully, because in everyday life treatment is usually given without prior qEEG testing (Table 3).
Stimulants (i.e. methylphenidate and dexamphetamine) act as noradrenaline and dopamine reuptake inhibitors (NARI & DARI). They therefore prevent the recycling of dopamine into the presynaptic vesicles, so that more dopamine is available for the transmission of the signal to the postsynaptic receptors and the ADHD-related dopamine deficiency is compensated for.
Stimulants have the following characteristics: They have response rates of up to 80%, a very rapid onset of action (30 min after ingestion), hardly any interactions and no development of dependence.
Serotonin syndrome is repeatedly mentioned in the interaction programs; this is so rare that stimulants can be combined with antidepressants or triptans without any problems. The side effects are limited to the noradrenergic effect with an increase in blood pressure and pulse rate as well as appetite and sleep disorders and rarely tic development. Symptoms of depression (“being extinguished”) or headaches are usually the expression of a relative overdose. In general: the dosage is not dependent on body weight, but should be individually titrated for each person, because there are very fast and very slow metabolizers! Blood level measurements are unnecessary. On the other hand, stimulants can be abused as neuroenhancers or – if snorted or injected – have the same effect as cocaine; they are therefore subject to narcotic prescription.
Night breaks are necessary so that the receptor systems can recover; this is v.a. Important in exam situations, as ADHD people may have postponed their study time to the night before the exam due to procrastination. Without the night break of the stimulant, however, it no longer works the next day.
Methylphenidate
Methylphenidate is the first-line drug for ADHD. Due to the individual sensitivities mentioned above, it is worth starting with a very low dose and slowly increasing the dose; weekly (telephone) contacts are useful for evaluation and dosage adjustment.
Although the short-acting methylphenidates Ritalin® and Medikinet® are not covered by health insurance for adults, it is worth starting medication with these substances (the cost price for patients is around CHF 15) because of the noticeable up and down effect.
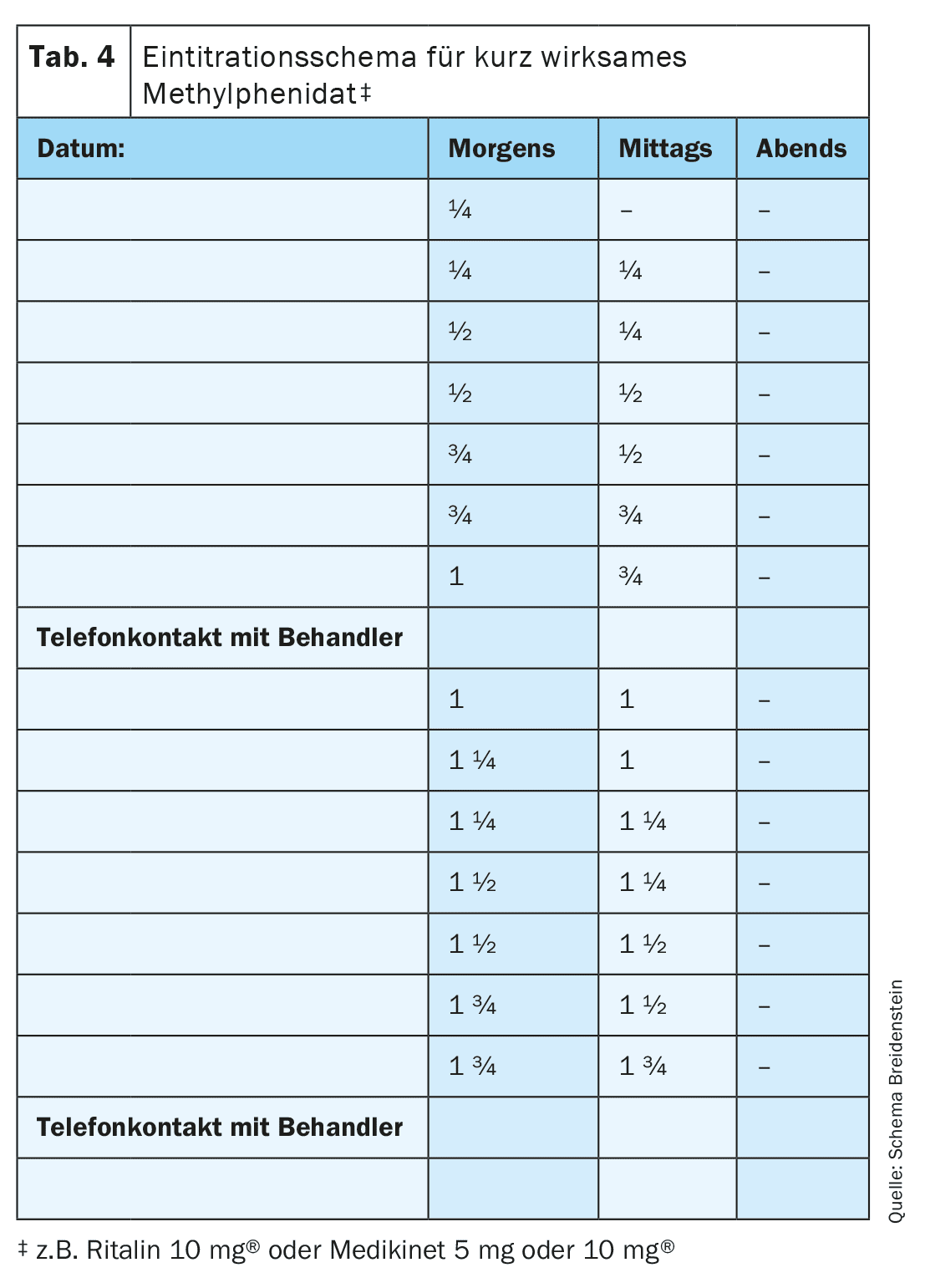
Increase according to the scheme in Table 4 until an effect is noticeable. Then give a maximum of ½ tbl. more per dose; if there are side effects or no increase in efficacy, reduce to a lower dose if necessary. Continue with the best dose or convert to a longer-acting preparation; even with intermittent intake, you can start directly with the “effective dose”.
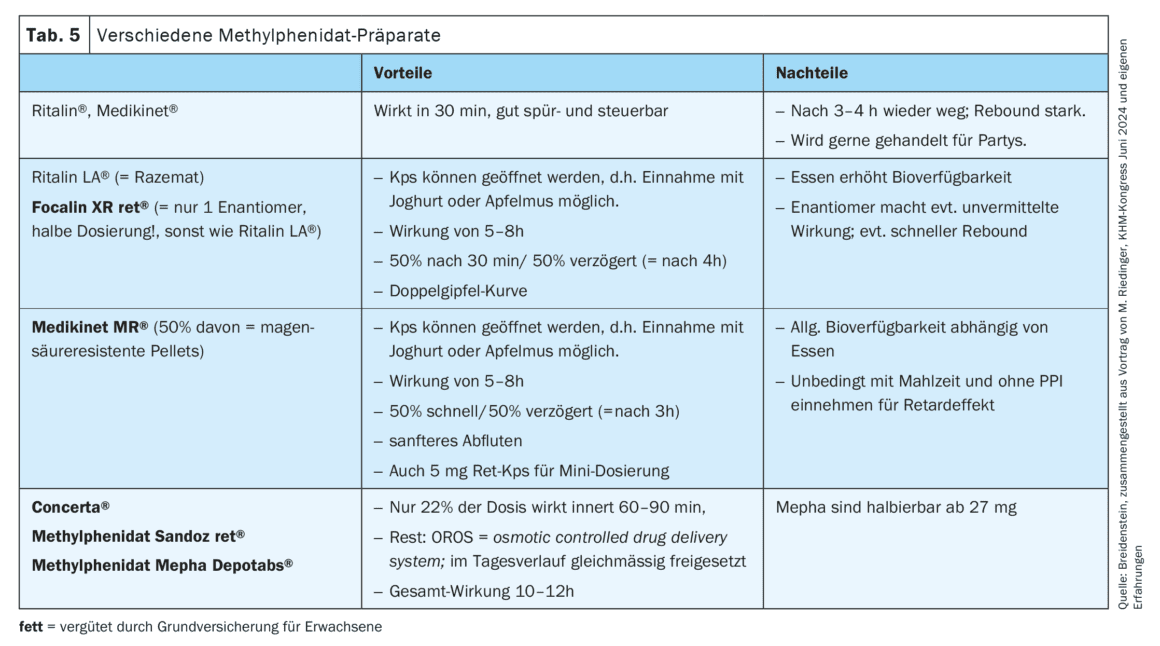
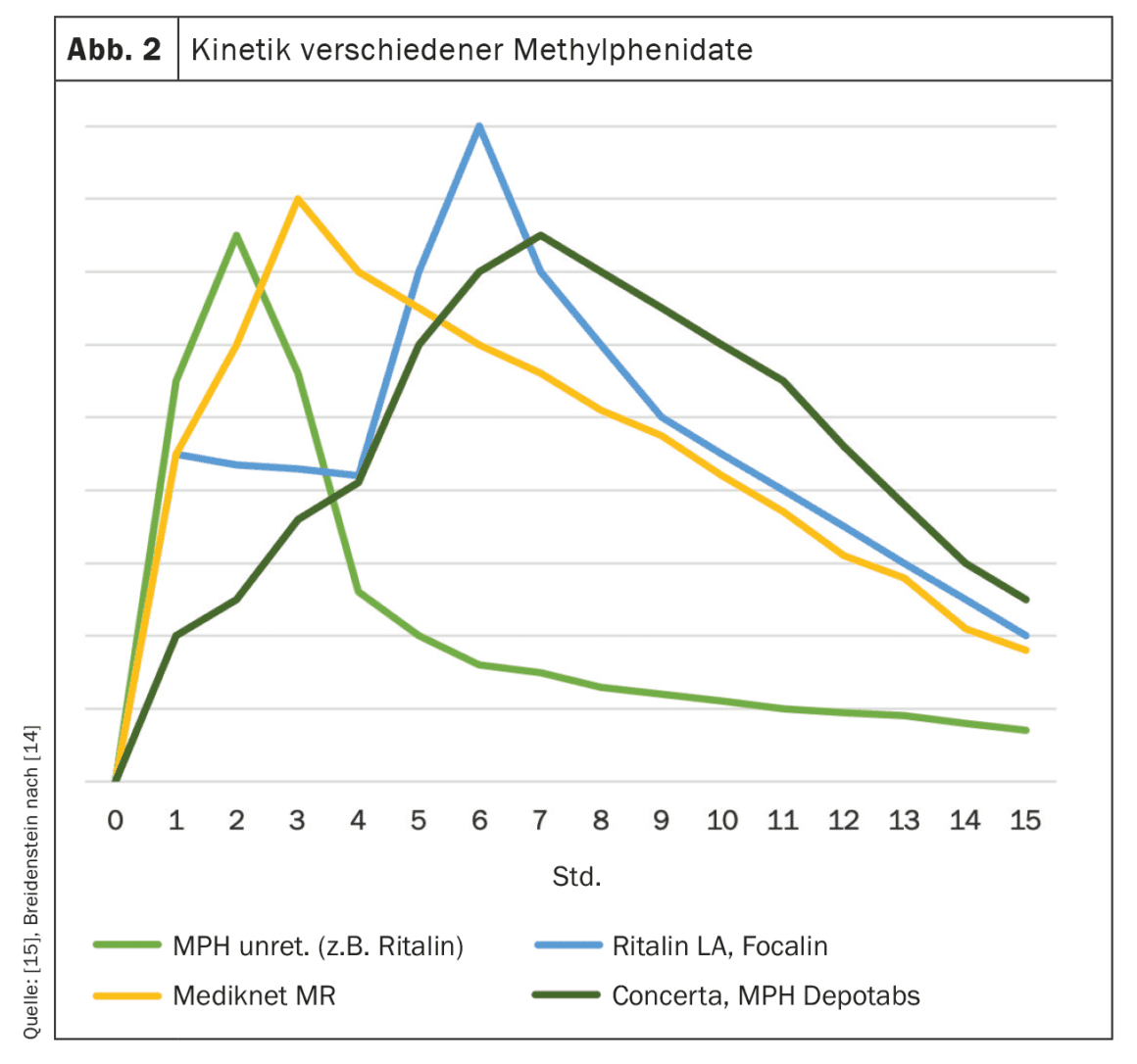
The various methylphenidates can all be interchanged and combined with each other (Table 5). Depending on the individual need (e.g. main effect time in the morning for morning grouches or 12h need for long school days), they can be selected and adjusted according to the kinetics; whereby the ordinate cannot be seen quantitatively) (Fig. 2) [14]. Interestingly, the tablet excipients also appear to influence the effect, so that the dosage may also have to be adjusted when switching to a preparation from another company. It therefore makes sense not to simply adopt the previous dosage 1:1, but to start with a slightly lower dosage and work your way up according to the patient’s feedback. On the other hand, the dosages specified in the drug compendium sometimes deviate considerably from individual requirements (this may affect the dose and dosage interval); a very participatory approach to medication determination is worthwhile here.
Only the preparations marked in bold in Tables 5 and 6 are reimbursed for adults. Sometimes, however, the health insurer must first be informed that they should not simply remove it from the invoice; other insurers at least require a doctor’s report to justify the indication…
Second-line preparations
If methylphenidate does not work, is not well tolerated or there is another additional indication, the following second-line preparations can be tried (Table 6): Dexamphetamine has a similar effect to methylphenidate, but has an additional vesicular release of dopamine and noradrenaline, so it is worth trying. To obtain smaller dosing intervals when titrating, the Lis-Dexamphetamine capsule can be dissolved in water and the appropriate proportion of the solution drunk (the rest goes in the fridge). As with methylphenidate, dexamphetamine can be used intermittently. Since, according to the list of specialties, the initial prescription must be issued by a psychiatrist, the prescription may require a psychiatrist consultation, depending on the health insurance company.
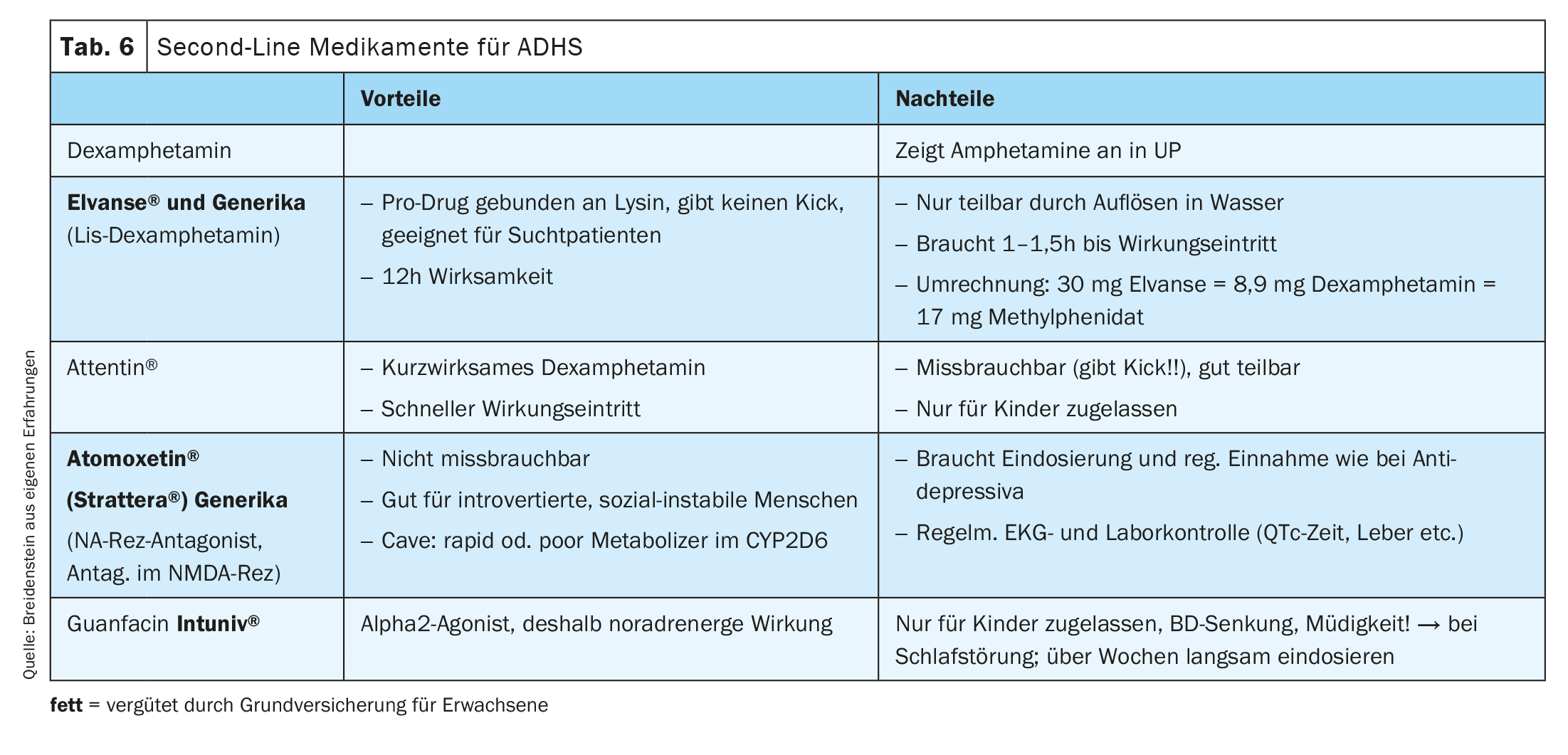
With atomoxetine or guanfacine, there is a need for continuous intake, the effect is not so immediate, so that a longer dosing process over several weeks is necessary, and quarterly to half-yearly ECG and laboratory checks must also be carried out. This is in contrast to stimulants, which can be taken as required, e.g. only on school or work days, and for which no additional checks are necessary (except for growth in children, as the reduction in appetite may lead to reduced calorie intake; and blood pressure checks in adults).
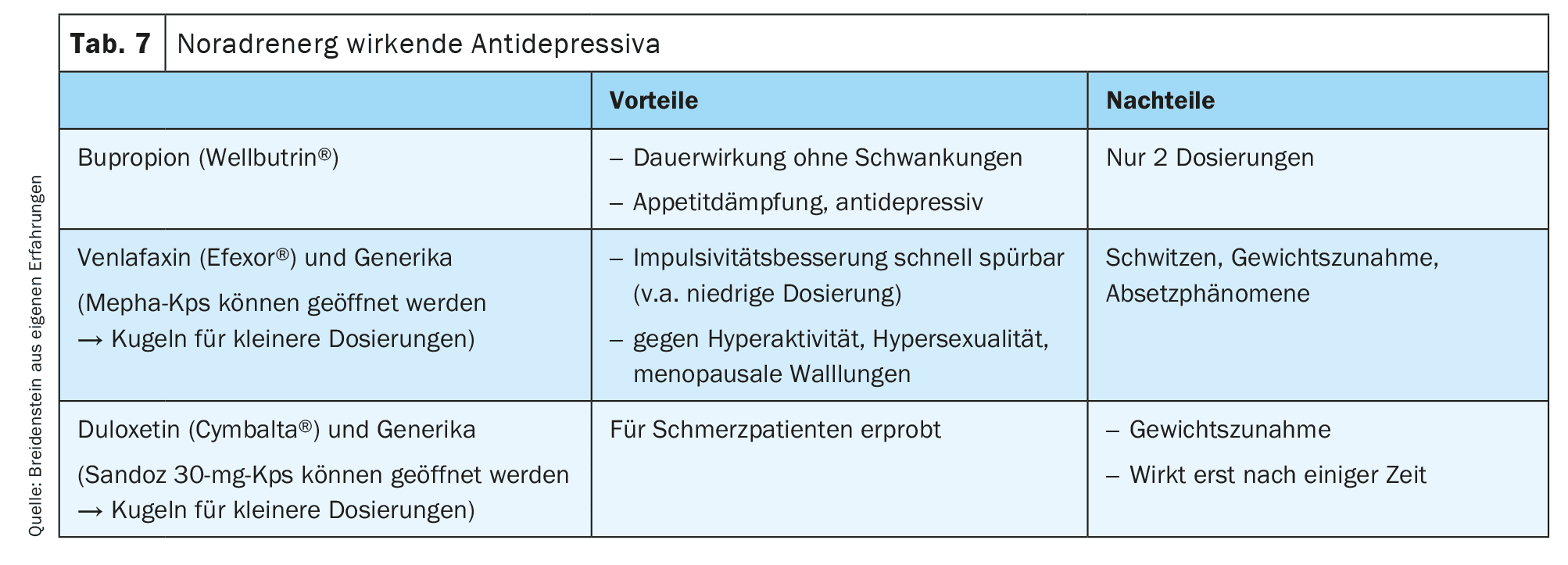
Noradrenergic antidepressants (noradrenaline reuptake inhibitors)
In adults with comorbidities, it is also possible to start with certain noradrenergic antidepressants (e.g. bupropion, venlafaxine or duloxetine) or combine them with stimulants. Antidepressants do not have the disadvantage of stimulants that there is no effect in the evening, but they often have significantly more side effects than stimulants (Table 7).
In the case of mild depression, ADHD should be treated first with long-acting stimulants; in the case of moderate to severe depression and ADHD: first treat the depression, then use stimulants (a combination of both substance groups is possible, however).
Take-Home-Messages
- People with ADHD are exciting and often very suffering patients who can be helped effectively.
- The multimodal treatment of ADHD in the GP manner is
- very necessary, satisfying and systemically relevant (entire family systems depend on it).
- Don’t be afraid of your own experiences with medication with stimulants and/or noradrenergic antidepressants; with a participatory approach with patients, little can go wrong – and you can always stop taking medication.
Literature:
- Spencer TJ, Biederman J, Mick E: Attention-deficit/hyperactivity disorder: diagnosis, lifespan, comorbidities, and neurobiology. J Pediatr Psychol 2007; 32(6): 631-642; doi: 10.1093/jpepsy/jsm005.
- https://chadd.org/about-adhd/general-prevalence-adults/#:~:text=General %20Prevalence%20of%20ADHD%20in%20Adults%201%20Prevalence,status% 3A %200%20percent%20reside%20in%20metro%20areas%20.
- Moffitt TE, Houts R, Asherson P, et al: Is adult ADHD a childhood-onset neurodevelopmental disorder? Evidence from a four-decade longitudinal cohort study. Am J Psychiatry 2015; 172(10): 967-977; doi: 10.1176/appi.ajp.2015.14101266.
- www.adhs.info/fileadmin/redakteure/zentrales-adhs-netz/ASRS_1.1._ADHS.pdf.
- Katzman MA, Bilkey TS, Chokka PR, et al: Adult ADHD and comorbid disorders: clinical implications of a dimensional approach. BMC Psychiatry 2017; 17(1): 302; doi: 10.1186/s12888-017-1463-3.
- Barkley RA: ADHD in Adults. Jones and Bartlett Publishers 2010; www.semanticscholar.org/paper/Attention-deficit-hyperactivity-disorder-in-adults-Barkley/632481c20ebffe65f5509fc5f565cf9572895bf2?utm_source=direct_link.
- Breidenstein E: ADHD in women, specific effect of hormones and menstrual cycle. J Gynecol Endocrinol 2022; CH25: 210-213; doi: 10.1007/s41975-022-00254-y.
- Purper-Ouakil D, Ramoz N, Lepagnol-Bestel AM, et al: Neurobiology of attention deficit/hyperactivity disorder. Pediatr Res 2011; 69: 69R-76R; doi: 10.1203/PDR.0b013e318212b40f.
- Quintero J, et al: Molecular Characterization of the Mechanism of Action of Stimulant Drugs Lisdexamfetamine and Methylphenidate on ADHD Neurobiology: A Review. Neurol Ther 2022; 11(4): 1489-1517; doi: 10.1007/s40120-022-00392-2.
- Breidenstein E: Diet for ADD/ADHD – cold coffee. Pediatrics 2005; 4: 1012; www.rosenfluh.ch/media/paediatrie/2005/04/Diaet-bei-ADSADHS-kalter-Kaffee.pdf.
- Yde Ohki CM, Walter NM, Bender A, et al: Growth rates of human induced pluripotent stem cells and neural stem cells from attention-deficit hyperactivity disorder patients: a preliminary study. J Neural Transm 2023; 130: 243-252; doi: 10.1007/s00702-023-02600-1.
- Lahrtz S: How ADHD and being a boss go together. NZZ from 13.02.2017.
- Neurofeedback lecture on 21.3.2017 at the ADHD Quality Circle Zurich (headed by Prof. Dr. D. Eich-Höchli), lecturer Ms. Susanne Grether, neuropsychologist and lecturer at Schoresch Competence Center for Bio- and Neurofeedback.
- Banaschewski T, Coghill D, Santosh P, et al: Long-acting medications for the hyperkinetic disorders. A systematic review and European treatment guideline. Eur Child Adolesc Psychiatry 2006; 15(8): 476-495; doi: 10.1007/s00787-006-0549-0.
- Lenhart S: ADHD – Often underestimated in adults. Pharmazeutische Zeitung from 21.04.2019; www.pharmazeutische-zeitung.de/bei-erwachsenen-haeufig-unterschaetzt.
HAUSARZT PRAXIS 2025; 20(1): 4–10









