
Respiratory allergies, especially allergic rhinoconjunctivitis, are very common. They primarily affect the 10-30 age group, but often limit the quality of life much more sensitively in older patients. The main triggers are: Pollen, animal epithelia, house dust mites, mold spores, occupational substances. Diagnosis is based on typical history and clinic, skin testing, and laboratory determinations by detection of specific IgE (increasingly at the molecular level). The three pillars of therapy are: Allergen reduction, pharmacotherapy and, for more severe symptoms, allergen-specific immunotherapy (hyposensitization).
Respiratory allergies are common and affect a good third of the population. Pollinosis alone affects up to 20% of the population. If these were infectious diseases, one would speak of an actual epidemic. Respiratory allergies occur more frequently between the ages of 15 and 30, but they can manifest themselves earlier, for example in infants. Pollen allergy can, for example, lead to measurably lower school grades in those affected and is by no means a trivial matter from this point of view. In older persons, respiratory allergies are rarer overall, but the patients often suffer much more from the corresponding symptoms. There has been a significant increase in recent decades. Possible causes include genetic predispositions, changes in lifestyle with altered microbial load and dietary habits, as well as climatic influences and increased allergenicity of pollen and other allergens. increased sensitivity of the respiratory tract to environmental pollutants plays a role. In this article, we would like to present basic information on the clinic, diagnosis and treatment of respiratory allergies on the one hand, and selectively highlight some new insights on the other hand.
The clarification of inhalation allergies
The clarification is based on the following points:
- Anamnesis and clinic
- Skin testing, in the vast majority of cases by means of prick tests
- Determination of specific IgE antibodies against single or panels of allergens
- in unclear cases, provocation tests conjunctival or nasal (e.g. in case of occupational allergies; in case of discrepancy between anamnesis and skin tests or specific IgE; in studies).
Anamnesis and clinic
Typical symptoms include rhinitis (with sneezing attacks more than three times in rapid succession, watery rhinorrhea, obstructed nasal breathing, and nasal pruritus), conjunctivitis (pruritus, redness, lacrimation, and mild photophobia), and bronchial asthma. Nasal obstruction over a prolonged period of time is often accompanied by a diminished or even abolished sense of smell (hypo-/anosmia) – a symptom and sign of nasal obstruction that patients usually find very bothersome.
While conjunctivitis and rhinitis tend to be reported in younger patients, asthma usually occurs later in the course (“floor change”) in about a quarter of patients. This often manifests simply as increased cough or mild exertional dyspnea as a sign of bronchial hyperresponsiveness. In about 15-25% of patients, associated food allergies due to cross-reactivity among molecularly related structures are present in addition to the symptoms mentioned above. These often manifest themselves mainly as oral complaints (pruritus, burning, slight swelling) when eating the corresponding foods (e.g. apples, nuts) – due to the heat and gastric sensitivity of the allergens rather exceptionally as anaphylaxis.
Allergen specific symptoms
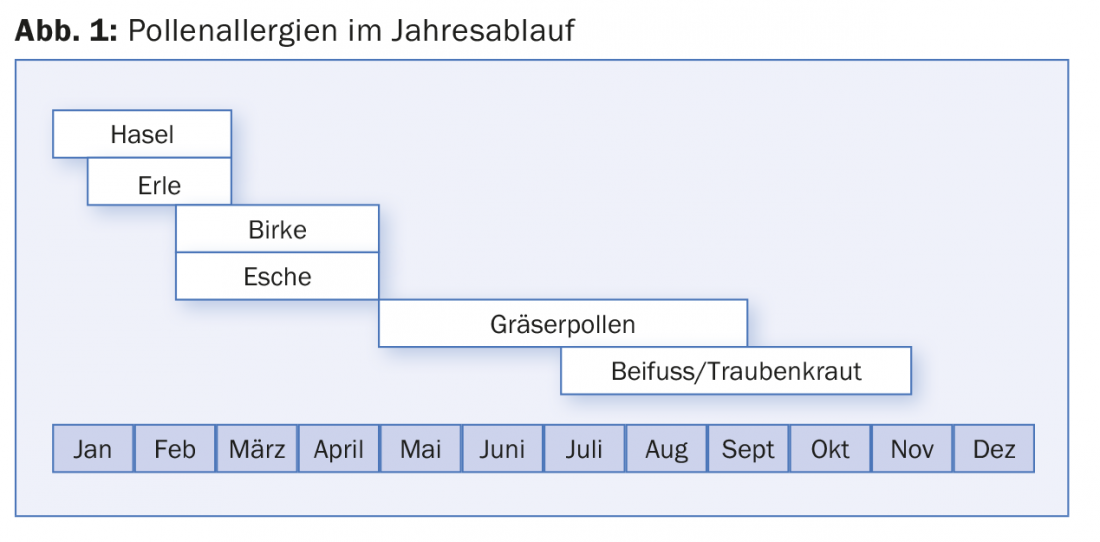
Seasonal allergens: Typical is also the strictly seasonal occurrence of symptoms according to the respective flowering time and usually intensified in sunny windy weather. As a rule of thumb, tree pollen are the triggers in spring, grass pollen in early summer and herbs in late summer (Fig. 1) . Changes in climatic conditions, new mining methods and newly imported plants can lead to quite significant changes in the pollen count. For example, we were able to show that a hybrid of the alder, so-called purple alder, which partly originates from Siberia, blooms in our latitudes up to two months earlier than the native alder and can thus already trigger hay fever symptoms at Christmas time.
Perennial allergens: In the case of year-round symptoms, dust mites and especially hairy pets such as cats, dogs or guinea pigs are the most likely allergen sources. Dust mites are found mainly in the mattress and pillow, the allergen is found among other things in the feces and thus goes as dust into the environment. House dust mite allergies therefore typically manifest themselves in the morning upon awakening and often more strongly in the winter half-year and heating period, due to less ventilation. In the case of actual animal allergies, the complaints usually occur during direct contact and can be easily attributed. In addition, rarer triggers such as houseplants (e.g. Ficus benjamina) or fish food (red mosquito larvae, in dry food for aquarium fish) as well as occupational allergens such as flour, flowers, isocyanates should also be considered. Mold spores can cause discomfort seasonally in outdoor air in late summer (Alternaria) as well as year-round in moldy indoor environments (Fig. 2).

Skin testing
The primary method of clarification for inhalation allergens is the prick skin test. According to the triggers, about eight to ten allergens are usually sufficient: pollen of birch, ash, grass and mugwort, one to two house dust mites, dog, cat hair and at most one to two further animal allergens (e.g. horse, guinea pig). Mold spores are also of importance, but are tricky in the prick test because of often insufficiently standardized extracts. In addition, a positive control (histamine, codeine) and negative control (NaCL) must also be tested. Very detailed instructions on how to perform the prick skin test can be found at www.ck-care.ch/merkblatter.
Laboratory determinations
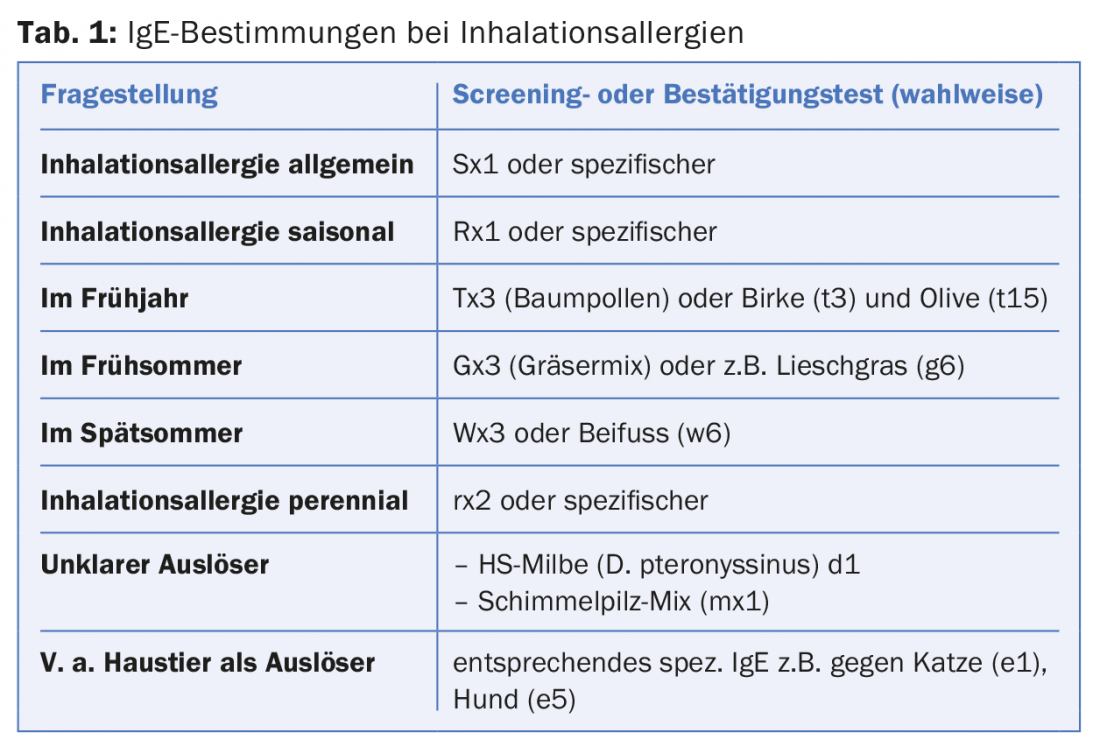
Alternatively or in addition to skin testing, specific IgE against a panel of allergens or individual allergens can be determined in serum. Advantages over skin tests here are the independence from drugs such as antihistamines and objective values, disadvantages are the latency until the results are available, the higher cross-reactivity and, especially with multiple tests, the higher costs. A compilation of the most important search and confirmation tests can be found in Table 1.
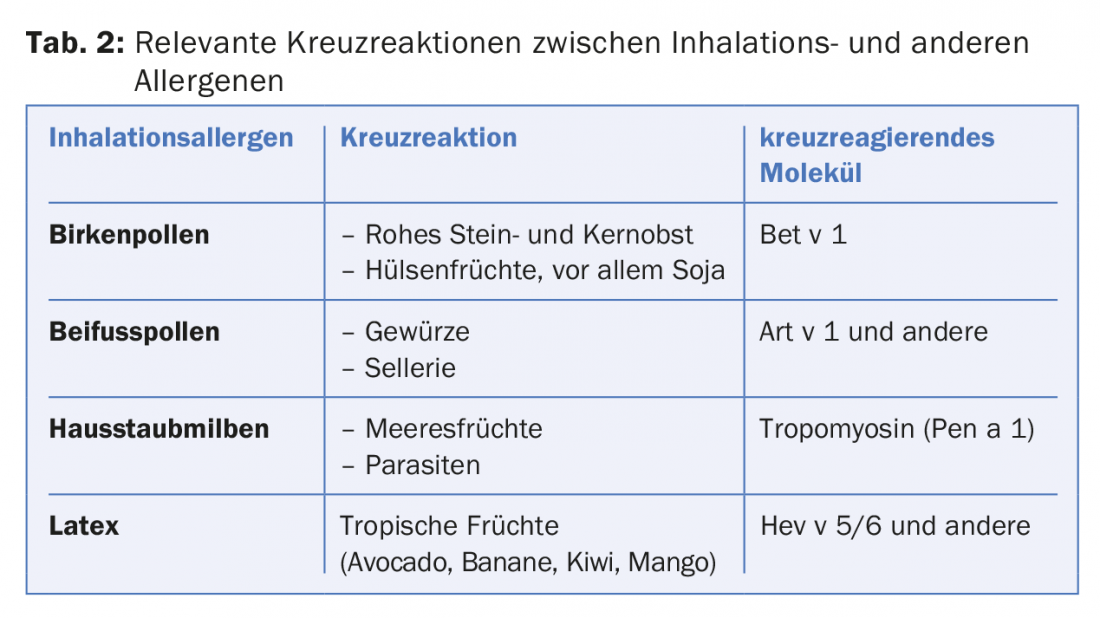
A major advance in the identification of sensitization pathways and, in some cases, factors for risk evaluation has been made in recent years by the determination of IgE at the molecular level. This approach is called molecular allergy diagnosis or component-based diagnosis (CRD for short). Here, for example, specific IgE against the main allergen of birch (Bet v 1), grasses (phl p 1/5) or cat (Fel d 1) are determined. For example, cross-reactions (Tab. 2) among different pollens can also be explained by sensitization to profilins present in all plants (such as Phl p 12, Bet v 2, Ole e 2). Determination of major allergens can be achieved in the selection of extracts for immunotherapy or for more accurate detection of ash pollen allergy via the related allergen of olive pollen (Ole e 1).
Such molecular IgE measurements are also increasingly useful in animal dander allergies. Thus, patients with sensitization to cat dander are allergic to cats exclusively only if the IgE are directed against Fel d 1 only; however, if the IgE are directed against lipocalins, allergies to most hairy animals are to be expected. In turn, patients with sensitization to the dog allergen Can f 5 are allergic only to males but not to females (Table 1).
The treatment of respiratory allergies
The therapy is based on three pillars:
- Allergen avoidance
- medicinal, mostly symptomatic therapy
- allergen-specific immunotherapy.
Allergen avoidance: Recognizing the trigger is a first important step to avoid or at least reduce the corresponding contact, for example by purchasing encasings (mite-proof covers for mattress, pillow and comforter) in case of house dust mite allergy. In the case of pet allergies, the formerly almost strict prohibition has been relaxed to some extent in atopics. Without discomfort in one’s own pet, keeping the animal is often even better in order to be able to maintain the tolerance that has been built up. There are also indications that keeping a dog could even have a preventive effect against allergies under certain conditions.
Pharmacotherapy of inhalant allergies: A central role is played by oral antihistamines, also known as H1 blockers (AH1). Nowadays, mainly second- or third-generation non-sedating or barely sedating AH1s should be used, as they are less likely to impair sleep quality. With the older highly sedating antihistamines (such as clemastine or dimetindene), it was shown that, for example, children’s school performance dropped again by up to 10% in addition to their pollen allergy. The AH1 in drop form can be used with children as young as six years old, and in some cases as young as two years old or even earlier. Topical nasal steroids are also suitable, especially for rhinitic symptoms, and are very effective in addressing nasal obstruction when used for a sufficiently long time over several days. Combination products with additional topical H1 blockers exert their effect somewhat more rapidly, which may increase compliance. Topical vasomimetics are very rapidly effective but should be used only for short periods because of the threat of privinism.
On the eye, on the other hand, these can be used without any problems; mast cell stabilizers are also often very useful here. For asthmatic symptoms, inhaled betamimetics or steroids, leukotriene antagonists and, in severe allergic forms, the IgE antagonist omalizumab may be considered, depending on the extent and GINA (Global Initiative for Asthma) guidelines. Other biologics (anti-IL-5 or anti-IL-13) are in clinical trials and are expected to be used soon in certain subtypes of asthma.
Allergen-specific immunotherapy: Immunotherapy, also known as hypo- or desensitization, is the causative treatment for many inhalant allergies and is indicated for moderate to severe rhinoconjunctivitis and/or well-controlled asthma. In well-selected patients – here, in addition to precise anamnesis, molecular allergy diagnostics can often help – success rates of over 80% can be expected for pollen allergies. The amount of allergen used must be sufficiently high, and the importance of the adjuvant is also increasingly recognized. In addition to the proven subcutaneous immunotherapy, the sublingual form of application, especially in tablet form, has become established as an alternative in recent years (e.g., for grass pollen allergy). Even for allergies to house dust mites or animal epithelia, quite effective regimens are available today, currently still mainly on a subcutaneous basis. New approaches through improved adjuvants or other routes of application (epicutaneous, intralymphatic) are currently being intensively investigated in clinical trials and could at best optimize treatment duration or frequency.
Further reading:
- Canonica GW, et al: A WAO – ARIA – GA²LEN consensus document on molecular-based allergy diagnostics. World Allergy Organ J 2013; 6(1): 17-29.
- Konradsen JR, et al: Allergy to furry animals: New insights, diagnostic approaches, and challenges. J Allergy Clin Immunol 2015; 135(3): 616-625.
- Imhof K, et al: Ash pollen allergy: reliable detection of sensitization on the basis of IgE to Ole e 1. Allergo J Int 2014; 23(3): 78-83.
- Chung CH, et al: Cetuximab-induced anaphylaxis and IgE specific for galactose-alpha-1,3-galactose. N Engl J Med 2008; 358(11): 1109-1117.
- Roduit C, et al: Development of atopic dermatitis according to age of onset and association with early-life exposures. J Allergy Clin Immunol 2012 Jul; 130(1): 130-136.
- Pfaar O, et al: Guideline on allergen-specific immunotherapy in IgE-mediated allergic diseases. Allergo J Int 2014; 23: 282-319.
- Gassner M, Gehrig R, Schmid-Grendelmeier P: Hay Fever as a Christmas Gift. N Engl J Med 2013; 368(4): 393-394.
- Wüthrich B, et al: Prevalence of Atopy and Respiratory Allergic Diseases in Eldery SAPALDIA Population. Int Arch Allergy Immunol 2013; 162: 143-148.
Useful Web Links:
- Current poll data for Switzerland and abroad:
www.pollenundallergie.ch - Up-to-date info for patients/concerned persons:
www.aha.ch - Links to training and information material for allergology in primary care via the Christine Kühne Center for Allergy Research and Education CK-CARE: www.ck-care.ch
DERMATOLOGIE PRAXIS 2016; 26(3): 10-13









