A first-in-class BCMA-targeted antibody-drug conjugate for the treatment of multiple myeloma in heavily pretreated adult patients who experienced disease progression during their last therapy has been approved in Switzerland since June 2022 and has been subject to health insurance coverage since November 2022 (1, 2). Outpatient treatment with monotherapy demonstrated a profound and durable response and a manageable safety profile in the pivotal trial (3, 4).
Multiple myeloma (MM), which belongs to the B-cell lymphomas, constitutes approximately 10% of all hematologic malignancies (5). Existing treatment options have allowed prolongation of overall survival (OS) of MM patients in recent years, but the emergence of resistant clones still frequently leads to treatment failure. With each subsequent treatment, the depth and duration of response reduce; a proportion of patients become refractory to proteasome inhibitors (PIs), immunomodulators (IMIDs), and monoclonal antibodies. These patients have limited treatment options and, with a median OS of 5.6 months, a poor prognosis (6). This reflects the urgent need for new therapeutic options with innovative mechanism of action (6). In the pivotal DREAMM-2 trial, the BCMA-targeted antibody-drug conjugate belantamab mafodotin (BLENREP) demonstrated a good and durable response in heavily pretreated, multiple refractory patients, especially as measured by the extent of pretreatment (3, 4, 7).
Profound and sustained response under BLENREP in the DREAMM-2 study.
In the multicenter, open-label, two-arm, phase II DREAMM-2 trial, 97 patients whose disease was progressive after ≥3 lines of therapy received 2.5 mg/kg BLENREP every 3 weeks as monotherapy until disease progression or unacceptable toxicity (3, 4). The overall response rate (ORR), which was assessed by an independent committee, was the primary endpoint and was 32% (31/97; 97.5% CI: 21.7%-43.6%) after a median 13-month follow-up(Fig. 1) (4). The majority (18/31; 58%) of these responders benefited from a very good partial remission (VGPR*: n=11) or an even more profound response (CR*, sCR*; n=7). Secondary endpoints included median duration of response (mDOR; 11 months [95% CI: 4.2-NE]) and expected median OS (13.7 months [95% CI, 9.9 months-not reached]) in the overall heme population. The response and survival of patients with risk-associated cytogenetics or renal insufficiency was comparable to the results of the overall population (4).
Monitoring for corneal changes
The most common adverse events with 2.5 mg/kg BLENREP were keratopathy (72%, severity ≥3 in 46%) and thrombocytopenia (38%, severity ≥3 in 22%). Corneal side effects led to treatment delay in 47% of patients but to permanent treatment discontinuation in only 3%. After 13 months, visual acuity changes had resolved in 82% of patients; no permanent visual loss was observed (4). To monitor side effects, an ophthalmologic examination is performed before starting treatment with BLENREP and before the first three subsequent cycles. Patients should also avoid contact lenses and regularly use preservative-free tear substitutes. Once moderate corneal side effects occur, adjust the dosage of BLENREP or delay treatment (1). Although dose modifications (delays or reductions) were frequently used for adverse event management in this study, they had minimal impact on response under BLENREP (4).
Conclusion
BLENREP has been approved in Switzerland since June 2022 and will be reimbursed by health insurers since November 2022 if the limit is met (1, 2). BLENREP is approved as monotherapy for the treatment of MM in heavily pretreated adult patients with at least four prior therapies who showed disease progression during the last therapy and whose disease is refractory to at least one proteasome inhibitor, one immunomodulator, and one anti-CD38 monoclonal antibody (1). Patients with a high degree of pre-treatment in particular can therefore now benefit from the effective and tolerable new treatment option.
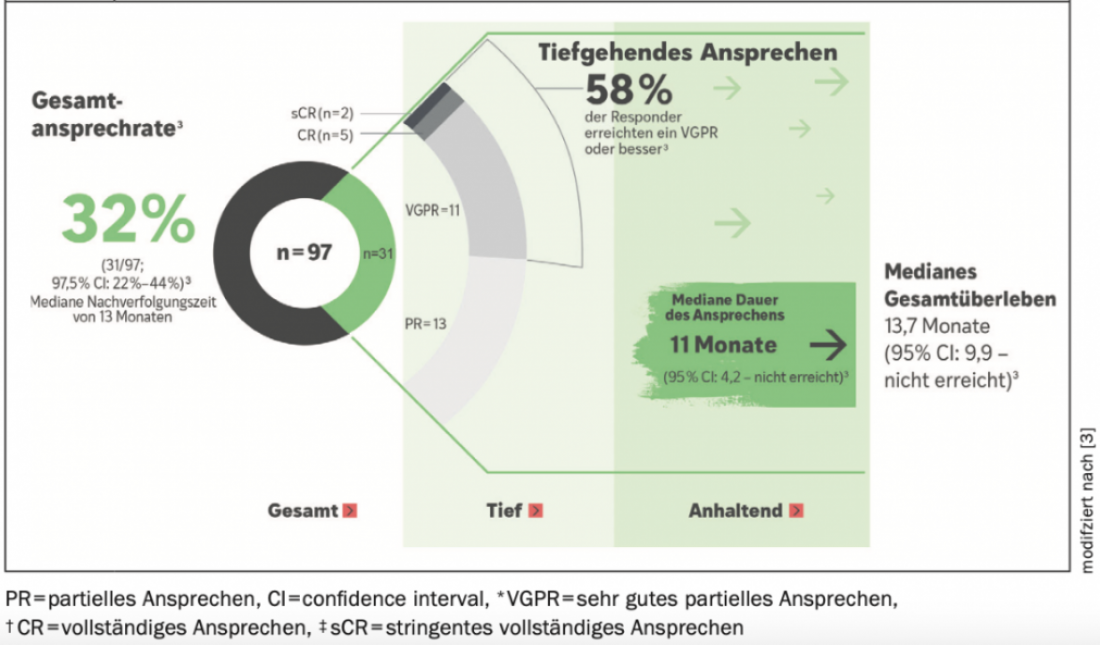
Figure 1: Response rates, duration of response, and overall survival in the DREAMM-2 trial of 2.5 mg/kg BLENREP at 13 months of follow-up. Adapted from (4).
————-
°BCMA = B cell maturation antigen, surface protein found exclusively on myeloma cells and plasma cells
*VGPR = very good partial response; CR = complete response; sCR = stringent complete response.
More information
Publireportage responsible for and financed by GlaxoSmithKline AG, Talstr. 3, CH-3053 Münchenbuchsee. Contact: +41 31 862 21 11
Trademarks are property of their respective owners. ©2022 GSK group of companies or its licensor.
Brief technical information BLENREP®
PM-CH-BLM-ADVR-220029-11/2022
Literature










