Histopathologically, infiltrates of histiocytes, numerous multinucleated giant cells, and few lymphocytes in the upper dermis are characteristic of this rare granulomatous disease. The present case underscores the importance of biopsy and histologic workup as diagnostic tools in dermatology.
Since 1975, anular elastolytic giant cell granuloma has been discussed as a distinct clinical picture distinguishable from necrobiosis lipoidica and granuloma anulare [1]. Since this granulomatous disease of unclear etiology often affects UV-exposed skin areas, it was initially referred to as actinic granuloma – the now internationally used term ” annular elast olytic giant cell granuloma” goes back to Hanke et al. back [2]. The etiopathogenesis has not been clarified to date. It is suspected that the elastic fibers develop antigenic properties through sunlight or other mechanisms, inducing a T-cell-mediated granulomatous inflammatory response [3].
Medical history and clinical examination
A 72-year-old patient presented to the outpatient clinic of the University Medical Center Mainz with erythematous, anular, partly garland-like marginal plaques with central fading and discrete fine lamellar scaling on the décolleté and upper back that had been present for about 6 months [4]. There was no itching or pain. He had already been treated with topical steroids, which did not result in healing. Pre-existing conditions included a history of chronic spinal pain syndrome due to multiple spondylodeses. The existing medication had been taken for years. Laboratory chemistry tests of venous blood were performed, and sample biopsies were also taken for further diagnosis. Furthermore, skin scales were examined mycologically.

Histological findings
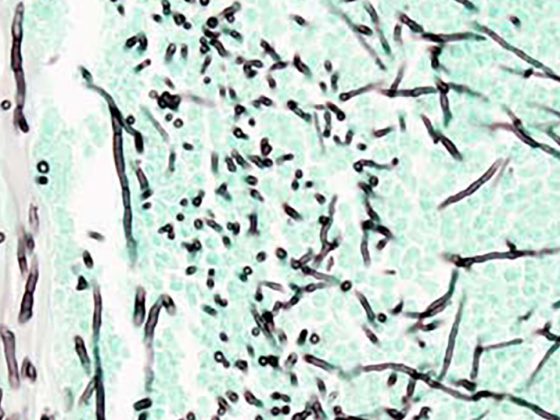
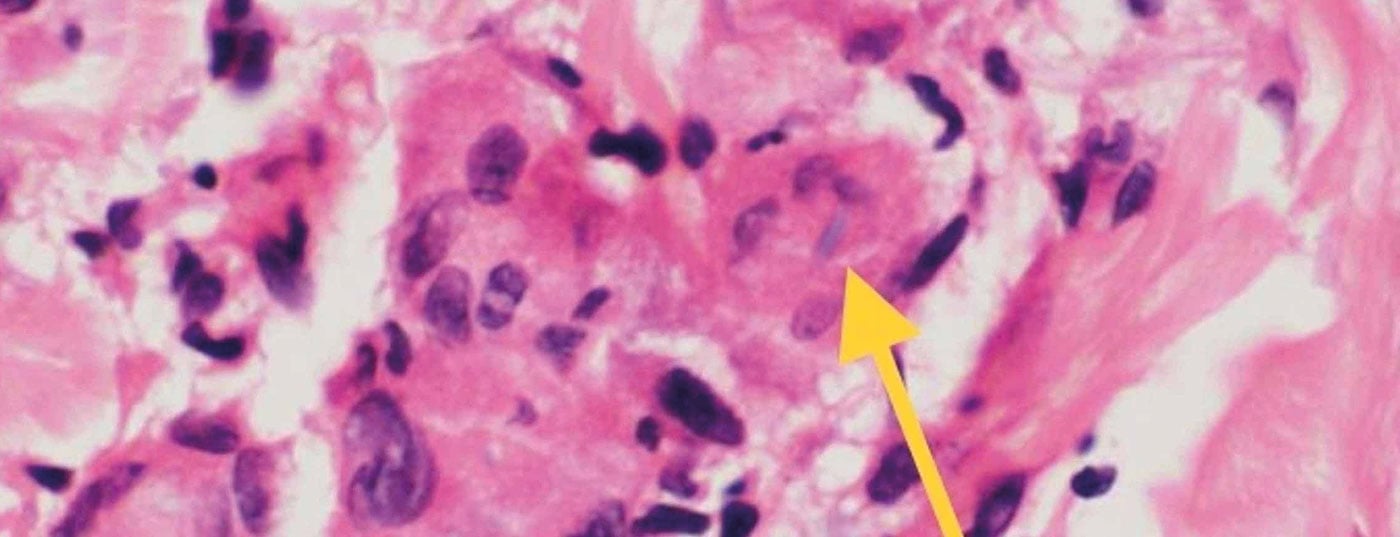
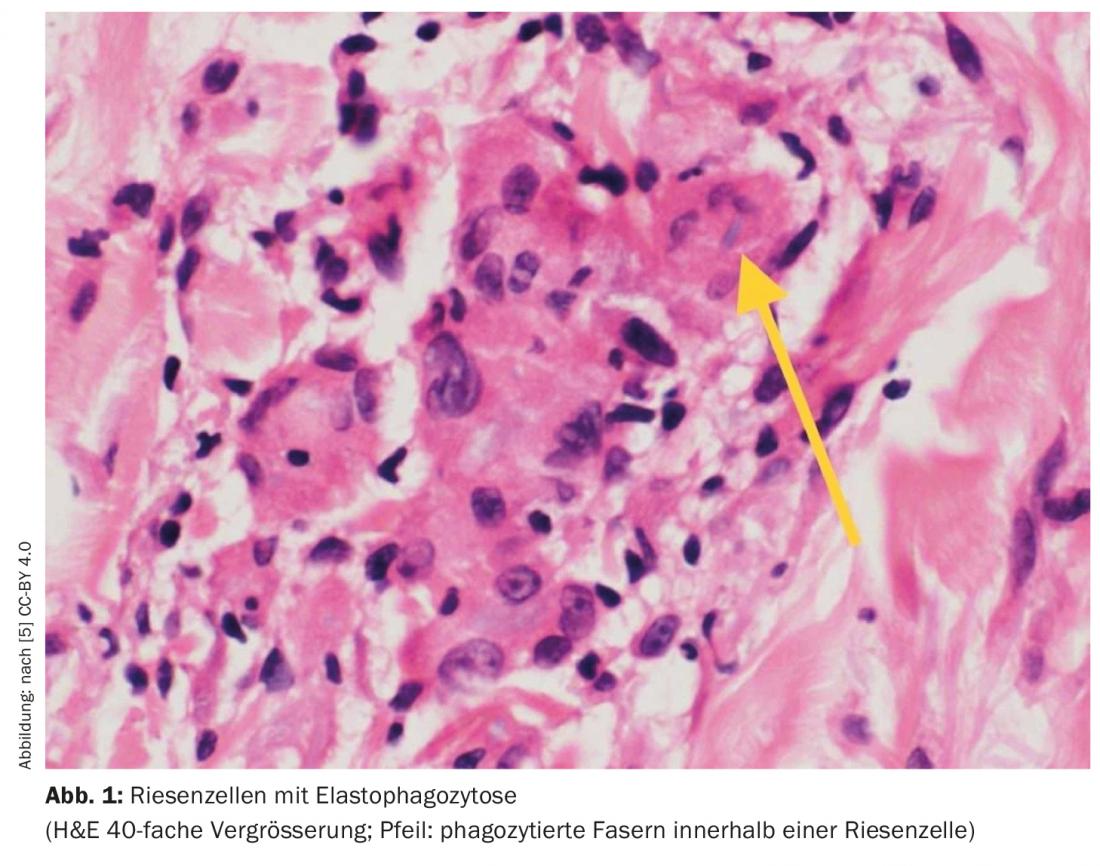
Histologically, there were superficial palisade granulomas with evidence of elastophagocytosis [4]. Characteristic of anular elastolytic giant cell granuloma is the complete absence of elastic fibers in the center of the lesions, whereas they are fragmented in the peripheral region and phagocytosed by histiocytes and giant cells. This elastophagocytosis is considered diagnostically conclusive [1]. Therefore, in conjunction with the clinical picture, the diagnosis of anular elastolytic giant cell granuloma was made in the present case [4]. Direct immunofluorescence showed no evidence of autoimmune dermatosis. Laboratory chemistry showed slightly elevated serum amyloid A and C-reactive protein. Rheumatology, autoantibodies, and ACE were unremarkable, as was mycological PCR.
Discussion
In anular elastolytic giant cell granuloma, there are usually solitary foci, but these can also occur over a large area, as in the present case. Differential diagnosis should consider other granulomatous diseases such as sarcoidosis and necrobiosis lipoidica, but autoimmune diseases such as cutaneous lupus erythematosus should also be ruled out [4]. Comorbidities documented in the literature include malignant hematologic disorders, diabetes mellitus, and arteritis temporalis. Therapeutically, topical or intralesional steroids may be sufficient for smaller lesions; systemic therapies such as dapsone or Quensyl are used for larger findings.
Literature:
- Kolde G: Granulomatous dermatoses. Current Dermatology 2014; 40(05): 193-204.
- Hanke CW, Bailin PL, Roenigk HM: Annular elastolytic giant cell granuloma. J Am Acad Dermatol 1979; 1: 413-421.
- O’Brien JP, Regan W: Actinically degenerate elastic tissue is the likely antigenic basis of actinic granuloma of the skin and of temporal arteritis. J Am Acad Dermatol 1999; 40: 214-222.
- Lang B, et al: The rare case: anular elastolytic giant cell granuloma. Diaklinik, DK02/02, JDDG | 1610-0379/2022/20 (Supp. 1) 1-49.
- Mistry A, Patel R, Mistry M, et al: (November 12, 2020) Annular elastolytic giant cell granuloma. Cureus 12(11): e11456. doi:10.7759/cureus.11456.
- MOJ Gerontology & Geriatrics 2018 (3), https://medcraveonline.com/medcrave.org/index.php/MOJGG/article/view/6981/13158, (last accessed 04/11/2022).
DERMATOLOGY PRACTICE 2022; 32(2): 49