
Hyperhidrosis is a serious disease, as sufferers have a high level of suffering which can have a major impact on their quality of life. In addition, the number of unreported cases of the disease is high – sufferers often do not know that they suffer from hyperhidrosis. Our expert Oliver Kreyden, MD, spoke on TV in April about hyperhidrosis and its treatment options. Below you will find the treatise on the subject prepared for medical professionals.
It is difficult to find an exact definition of hyperhidrosis (HH) because the boundary between physiologic and pathologic sweating is blurred. Therefore, it is important to include the impairment of the quality of life (Quality of Life [QOL]) of the affected persons. According to one study, this is significantly limited in 80% of those affected. After therapy, axillary 75% and palmoplantar 50% of patients had no more limitation. The HH is due to the numerous studies with data of a considerable suffering resp. a serious restriction of the quality of life as a disease and to distinguish it from a lifestyle disease.
The therapy of first choice is called botulinum
If aluminum salts do not bring the desired success, the next step is botulinum therapy (Fig. 1a and 1b).
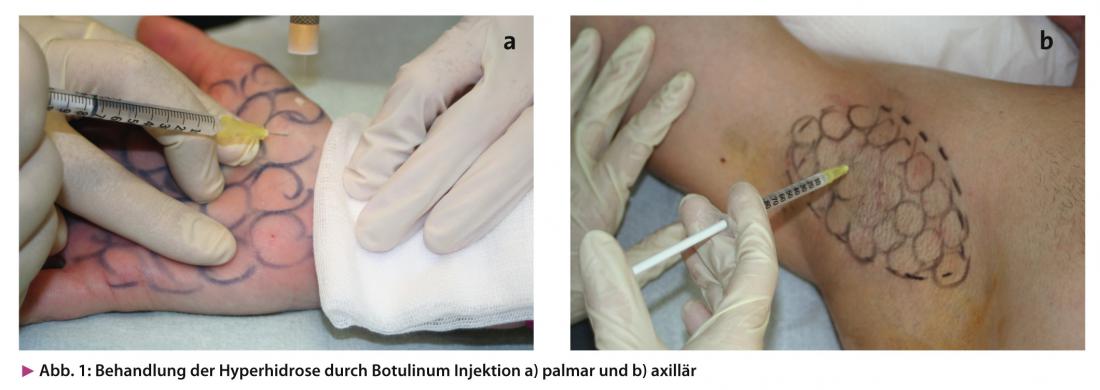
By a single treatment with setting of about 20 injections per treatment area, 90% of the patients can have their HH docked. The therapy lasts approximately six months, so interested patients can expect twice-yearly therapy.
Due to the specific mechanism of action as well as the exclusively local effect of the drug, no side effects in the actual sense (side effect!) are known. It is precisely this circumstance that makes this form of therapy so successful: benefit without problems! This was also the reason why the first hyperhidrosis consultation in Switzerland was founded in 1997 and was extremely successful (Kreyden Hyperhidrosis still runs this consultation).
This form of treatment is also extremely effective palmoplantar, although it is somewhat more complex and cost-intensive. In addition, this indication requires good training and a lot of experience on the part of the treating physician. While axillary treatment does not require any anesthesia, palmoplantar injections are painful. Kreyden Hyperhidrosis has developed a specific anesthetic technique that allows virtually painless treatment even in the area of the hands. Iontophoresis with 2 percent lidocaine solution is performed in advance. This brings a superficial anesthesia, which allows the targeted cryoanesthesia performed directly before each injection to be virtually painless. Due to the targeted cold anesthesia, in turn, the fine injections are hardly noticeable even on the palms of the hands and/or feet. In practiced hands, hands and/or feet can thus be treated with little pain within a few minutes without any significant problems. It was this technique that enabled the unhesitating extension of botulinum therapy beyond the axillary indication to the otherwise somewhat more difficultly classified palmar and even plantar treatment.
When is surgical treatment indicated?
Surgical solutions should only be considered after unsuccessful botulinum treatment, since the surgical forms of therapy are associated with considerable side effects and/or complications: insufficient effect after axillary suction curettage, scars with wound healing disorders after open axillary sweat gland excision, sometimes severe compensatory hyperhidrosis after thoracoscopic sympathectomy (TS). Compensatory hyperhidrosis after TS occurs in practically all patients who have undergone surgery, with increased sweating primarily lumbar and in the area of the inner thighs. However, the majority of those operated on do not find this compensatory sweating very distressing compared to before with the cold-wet hands. However, approximately 10% of TS patients experience massive sweating in multiple areas of the body after surgery. In these patients, appropriate therapy is difficult, as usually only anticholinergic systemic therapy with its various side effects remains. It is important that patients are made aware of this rare serious side effect after TS.
Minor’s welding test is indispensable as a good indicator
Minor’s welding test is a semi-quantitative measurement method for objectifying the amount of welding. The axilla is stained with Lugol’s solution (potassium iodide solution). Then the marked area is finely dusted with potato starch. Both Lugol’s solution and potato starch can be prepared by your pharmacist without any problems. Depending on the severity of the hyperhidrosis, the area changes to a different shade of purple (intensity). The extent of the HH also shows great variability (extent) (Fig. 2a-c).

Important prognostic statements can also be derived by means of Minor’s sweat test: In the case of strong, possibly even dripping coloration, it can be assumed that the effect of the treatment will last less long than in the case of weak, barely visible coloration. The test is cheap, easy to perform and can also be delegated. Thus, Minor’s sweat test is indispensable in the treatment of axillary hyperhidrosis. Consequently, one should perform the test – especially axillary!
HAUSARZT PRAXIS 2013; No. 6: 9-11









