Incomplete hippocampal inversion (IHI), also known as hippocampal malrotation, is a fetal developmental disorder with incomplete infolding of the fetal dentate gyrus, ammonic horn, subiculum, and parahippocampal gyrus [1]. In most cases, the IHI is unilateral and located on the left side. Bilateral IHI is very rare [1]. Concomitant cerebral developmental abnormalities are possible. IHI was initially described in patients with epilepsy or severe brain developmental disorders. However, recent studies show that IHI occurs with a frequency ranging from approximately 4% to 19% [1, 2] even in the healthy population, but mostly unilateral and incomplete. We report a case of bilateral complete IHI in a patient with epilepsy.
Case Report:
A 35-year-old female patient presented to our emergency department with severe headache. Personal history included migraine without aura and epilepsy since childhood. The latter manifested itself first of all at the age of eight months by febrile convulsions, which in the further course manifested themselves by generalized tonic-clonic seizures, absences and episodes with negative myoclonia (falls without loss of consciousness and without dropping objects). The clinical neurological examination was unremarkable on admission. The patient was on anticonvulsant therapy with primidone. Past EEG examinations had repeatedly revealed generalized epileptic activity with intermittent focal findings bitemporally and spike-wave patterns with a frequency of 3/second. Cranial imaging had not been performed previously.
MRI performed during the inpatient stay revealed bilateral IHI as the only abnormality.
Imaging:
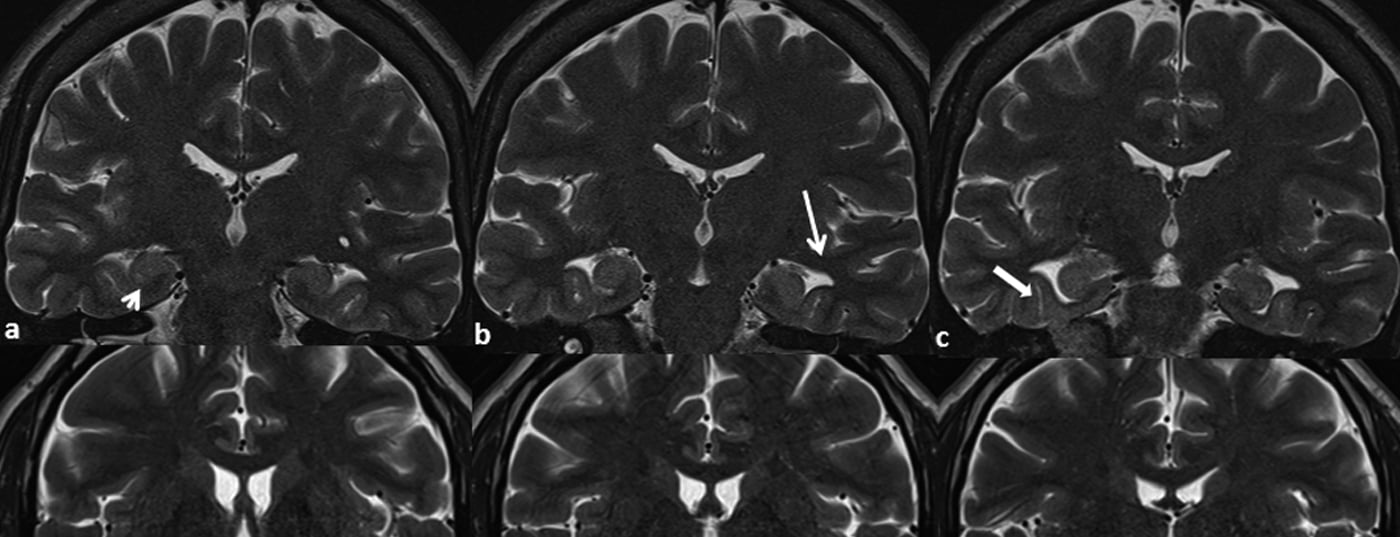
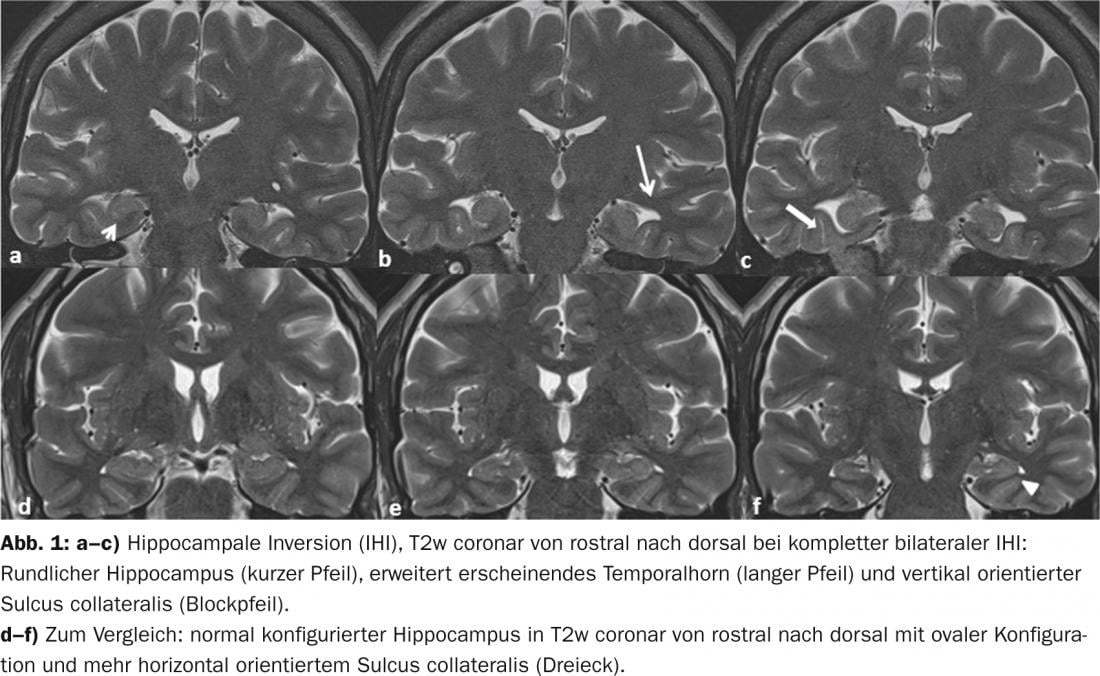
Coronal T2w images (Figs. 1a-c) show the typical signs of IHI from rostral to dorsal: roundishly configured hippocampus (short arrow) with normal signal behavior and volume, fuzzy internal structure of the hippocampus, dilated-appearing temporal horn (long arrow), and vertically oriented sulcus collateralis (block arrow) [1–3]. In comparison, the normally configured hippocampus of a healthy subject in the coronal T2w images (Fig. 1d-f) shows the typical oval shape (triangle) with narrow temporal horn and more horizontally oriented sulcus collateralis.
Discussion: Incomplete infolding of the hippocampal and parahippocampal structures results in a roundish or pyramidal hippocampal formation in coronal sectional plane. In IHI, the total hippocampal volume does not deviate from the norm, but the craniocaudal diameter is equal to or greater than the transverse compared with the normally rotated hippocampus. The temporal horn of the lateral ventricle thus appears dilated. The parahippocampal gyrus appears more vertically oriented due to incomplete infolding. IHI may extend along the entire hippocampus (complete) or affect only parts (partial) [2]. Our patient presents with a complete bilateral IHI.
Despite the structural abnormalities, IHI typically does not exhibit signal aging in T2w [3]. Although IHI appears to be associated with symptomatic epilepsy in most cases, recent literature evidence demonstrates that it can also manifest in healthy individuals without other cerebral developmental abnormalities [1].
Thus, the functional pathologic significance of IHI remains uncertain to date. Further scientific studies are therefore needed to more thoroughly define the pathological value of this entity.
Literature:
- Bajic et al: Incomplete Inversion of the hippocampus – a common developmental anomaly; Eur Radiol 2008.
- Bernasconi et al: Analysis of shape and positioning of the hippocampal formation: an MRI study; Brain 2005.
- Gamss RP, et al: Prevalence of hippocampal malrotation in a population without seizures. AJNR Am J Neuroradiol 2009.









