Driving aspects (driving competence) are not included in the mandatory driving fitness examination. Experience shows that the primary care physician is best at checking medical fitness to drive and an experienced driving instructor is best at checking driving competence.
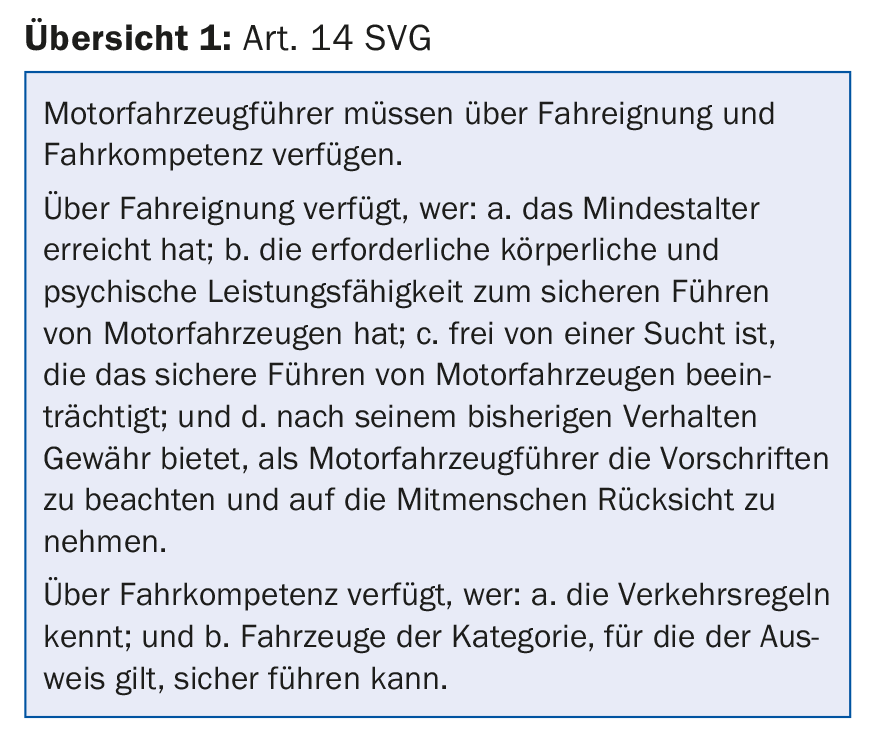
“Via sicura”, safety on the road, is a basic need of the population. The legislator regulates this in the Road Traffic Act. Art. 14 of the SVG states: “Motor vehicle drivers must be fit and competent to drive” (overview 1). I.e., both health and driving requirements are necessary for the driver’s license. The Traffic Licensing Ordinance VZV serves to enforce the law.
The innovations in the SVG and VZV created by “Via sicura”, which came into force on 1.7.2016, are tangential to the work of general practitioners when it comes to questions of driving ability assessment of older drivers.
How was it regulated in the past?
Already in the past it was noticed that certain old drivers steered their vehicles wrongly and unsafely, sometimes they were a real traffic obstacle and more often produced a traffic accident. For this reason, in 1976, the legislature decided that drivers over the age of 70 must undergo mandatory “driver’s license screening” (VZV Art. 27). A medical examination, which could also be carried out by the family doctor, was used to find out whether a driver was still “fit to drive”, i.e. whether he still possessed the prerequisites for driving a motor vehicle. If the minimum medical requirements were met, the cantonal road traffic office (SVA) issued the driver’s license for a further two years on the basis of the doctor’s certificate.
Evaluation of the medical screening
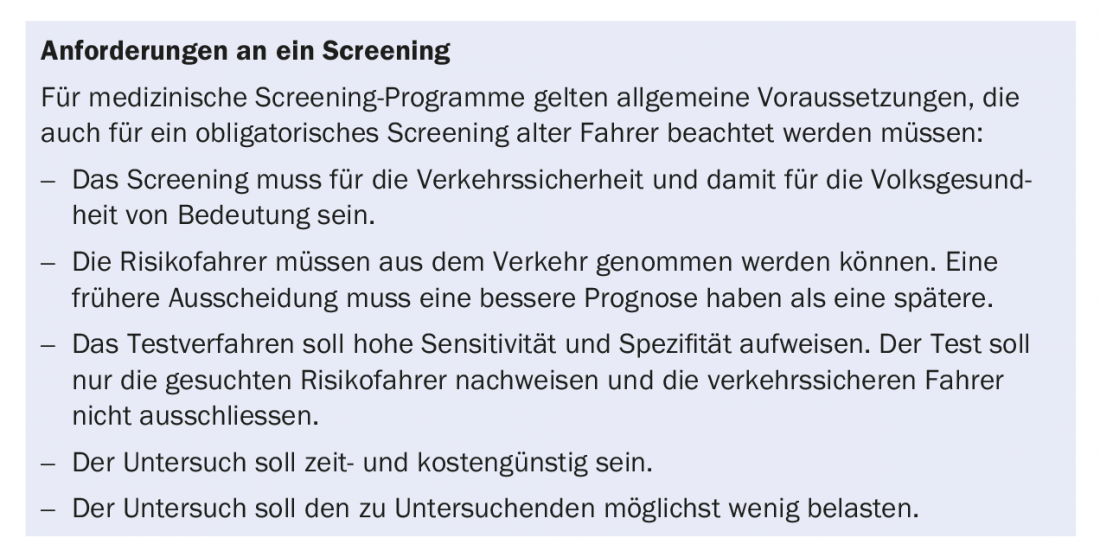
Unfortunately, no research has been conducted in Switzerland to determine whether mandatory medical screening from age 70 improves road safety. Numerous foreign studies, however, have evaluated age-related mandatory health screenings. A positive effect on traffic safety could not be demonstrated [3]. No improvement was obtained even with specifically cognitive testing procedures [4]. Rather, the screenings caused negative effects for seniors, particularly by switching to much more dangerous modes of traffic participation such as walking or bicycling [3].
Because in recent times the result of the obligatory driving fitness check seemed unsatisfactory also in Switzerland, specialists wanted to improve the screening. Regionally, the examinations were only allowed to be performed by district physicians or performed by physicians specially appointed by road traffic offices. It was not known whether traffic safety improved in these regions afterwards.
Since 1.7.2016, driving fitness checks have been standardized as part of the “Via sicura” amendment. As before, the organization of the controls and the decision on the driving license lie with the cantonal road traffic offices. There are now four levels of traffic medical examination, depending on the area of responsibility.
- Mandatory driver fitness screening for drivers 70 years of age and older is the lowest level 1 and is performed as before by primary care physicians resp. General practitioners performed.
- By referring traffic medicine complicated or unclear cases from level 1 physicians to level 3/4 physicians, the administration aims to improve the quality of driver fitness assessments and thus traffic safety.
- Level 2 physicians, in turn, are trained to perform traffic medical checks on drivers in higher categories [5].
The innovations are anchored in the SVG (Art. 15d) and in the VZV (Art. 5a, d, e, g, f). Art. 14 of the SVG as well as Art. 27 and Art. 34 (possibility of a driving license with restrictions) of the VZV remain unchanged.
Reflections on the current situation
Many measures aimed at improving road safety have been positively received so far. I am thinking of improvements to road infrastructures, driver assistance systems, speed limits, seat belts, alcohol restrictions, drug prohibition, etc. There is also a good aspect to the obligatory control of drivers over 70 years old. Although evidence of effect on traffic safety is lacking, the conversation between the primary care physician and the senior driver does raise awareness of the approaching decision to surrender the ID card [6]. It makes sense to standardize medical driver fitness checks and the corresponding cantonal forms. It is also useful that the primary care physician can refer a “problem case” to a higher-level office.
So, as before, the cantonal authority offers drivers over the age of 70 to undergo a medical examination for fitness to drive every two years (discussion: over the age of 75). The examination is uniform and limited to medical matters (VZV Art. 5i, Appendix 2 Examination copy for doctor, Appendix 3 Result report to the cantonal authority). The results are reported to the Road Traffic Authority: Visual acuity results, whether and what traffic-related diseases or conditions exist, whether the minimum medical requirements are met (Appendix 1 VZV), whether there is an unclear result and the definitive assessment should be carried out by a doctor of the higher qualification level, whether no vehicle should be driven due to doubts about the fitness to drive until further clarification. Possible conditions are: Glasses, regular medical check-ups with a level 1 doctor or a specialist doctor with reporting of results to the cantonal authority, but also blood glucose measurement before starting the journey in case of diabetes.
Critical and confidential reports to the authorities affect the relationship of trust between physician and patient, which is why family physicians occasionally refuse to perform mandatory driver fitness examinations. Art. 15 d SVG states that physicians are released from professional secrecy with regard to reports of doubted fitness to drive.
In turn, employees of the road traffic office check the medical data very carefully. If, from the official’s point of view, the certificate is incompletely answered or contains unclear formulations of diseases and conditions, the case is immediately forwarded to traffic medical higher authorities. Offices do not want to be guilty of anything and are expanding the administration [7]. The approach sometimes brings to mind Mark Twain’s quote, “And when they lost sight of the goal, their efforts were redoubled.”
False negative findings
And the goal actually seems to have been lost somewhat from sight. Because: If no relevant illnesses or conditions are present and the minimum medical requirements are met, there is “fitness to drive”. In contrast to the colloquial understanding of “being suitable for driving”, in the traffic medical sense only the fulfillment of certain required performances of body and mind is meant here. An old subject with very little driving routine or poor handling of his or her new car may have very poor practical driving skills despite being “fit to drive,” and would therefore be a high-risk driver not covered by the screening process and a burden on road safety.
False positive findings
Additional traffic medical clarifications arise if, for example, a test person had to undergo surgery for a cataract disease shortly before the mandatory driving fitness examination. In this case, there is an expected temporary inability to drive. In such cases, especially when polymorbidity is present, the authorities do not tolerate the postponement of the obligatory driving fitness test. Because of the current condition and the unresolved end result, there is then a threat of expensive additional checks, triggered by higher-level physicians who do not know the patient. The cost-effectiveness of mandatory screening is thus worsened. If a test person cannot pay the high special traffic medical costs including the additionally prescribed consultations with specialists, the examination is forfeited, resulting in the withdrawal of the driver’s license – if the screening with the general practitioner could have taken place three months later, the fitness to drive would probably have been confirmed. Bad luck that this subject was selected false positive. Should the individual later switch to a dangerous electric bike, the risk of accidents on the road is more likely to increase.
Returning to the goal of road safety
Mild short-term memory impairment combined with sometimes nocturnal disorientation may be signs of incipient dementia. In such a case, after the general practitioner has made the obligatory driving fitness examination and has affirmed the fitness to drive, should the traffic physician make an additional examination because of the report of the slight cognition disorder and possibly also obtain a neuropsychological opinion? In such a case, it would be much more targeted if, instead of additional medical examinations by level 3/4 physicians, the general practitioner were allowed to carry out the driving fitness examination more closely and, on his recommendation, the driving competence was additionally checked by the official driving expert (possibly accompanied by the traffic physician).
In old age, almost any serious illness can become relevant to traffic. In addition to specialist recommended driving suitability guidelines for epilepsy, stroke, Parkinson’s disease, microsleep, allergy and diabetes, guidelines for cardiovascular diseases, lung diseases, depression, psychosis and tumor diseases could soon appear. The expansion of traffic medical assessments seems almost limitless [7]. Is the actual goal of the investigation, “controlling the road safety of older drivers and thus reducing the number of accidents on the roads”, being lost because of all the medical driving fitness examinations?
Take-Home Messages
- Family physicians are sensitive to limitations in their patients’ fitness and competence to drive.
- The mandatory driver fitness examination is conducted exactly according to the new official guidelines. Driving aspects (driving competence) are not included. The medical driving decision should not be influenced by a driving competency finding.
- “Fitness to drive” is often only valid for a short time. In everyday practice, both health and driving requirements are discussed in a targeted manner when considering the question of responsible driving. Experience shows that the primary care physician is best at checking medical fitness to drive and the driving advisor – an experienced driving instructor who knows the difficulties seniors can have driving – is best at checking driving competency. Driving behavior control in real traffic, counseling and possibly driving lessons following the general health examination are important supports for the road safety of older drivers [1,2].
Literature:
- Seiler K: Driving advice close to practice – refreshing driving skills. L-drive 2014; 4: 4-6.
- Poschadel S: Trainability of driving competence of older drivers in real traffic. Presentation Switzerland. Driving Advisory Club 2016.
- Fastenmeier W, et al: Selection or empowerment: How to maintain mobility of older drivers? Position statement on behalf of the executive committee of the German Society for Traffic Psychology. Z f Verkehrssicherheit 2015; 1.
- Siren A, Meng A: Cognitive screening of older drivers does not produce safety benefits. Accident Analysis and Prevention 2012; 45: 634-638.
- Management and leadership of the Advanced Training Center for Driver Fitness Assessment Switzerland: Innovations due to Via sicura. Swiss Medical Journal 2015; 96: 1511-1514.
- Hausärzte Schweiz: Fahreignung von Personen über 70. Positionspapier von Hausärzte Schweiz zur period. med. Verification of fitness to drive. PrimaryCare 2011; 11(7): 103-105.
- Schedler K, Demaj L: Impact orientation – the behavioral dimension. Impacts of the University of St. Gallen 2015; 10: 12-15.
HAUSARZT PRAXIS 2017; 12(8): 41-43









