
Cardiovascular comorbidities in psoriasis may lead to a reciprocal influence of systemic therapies with implications for disease progression. Early detection and treatment are important factors in disease management
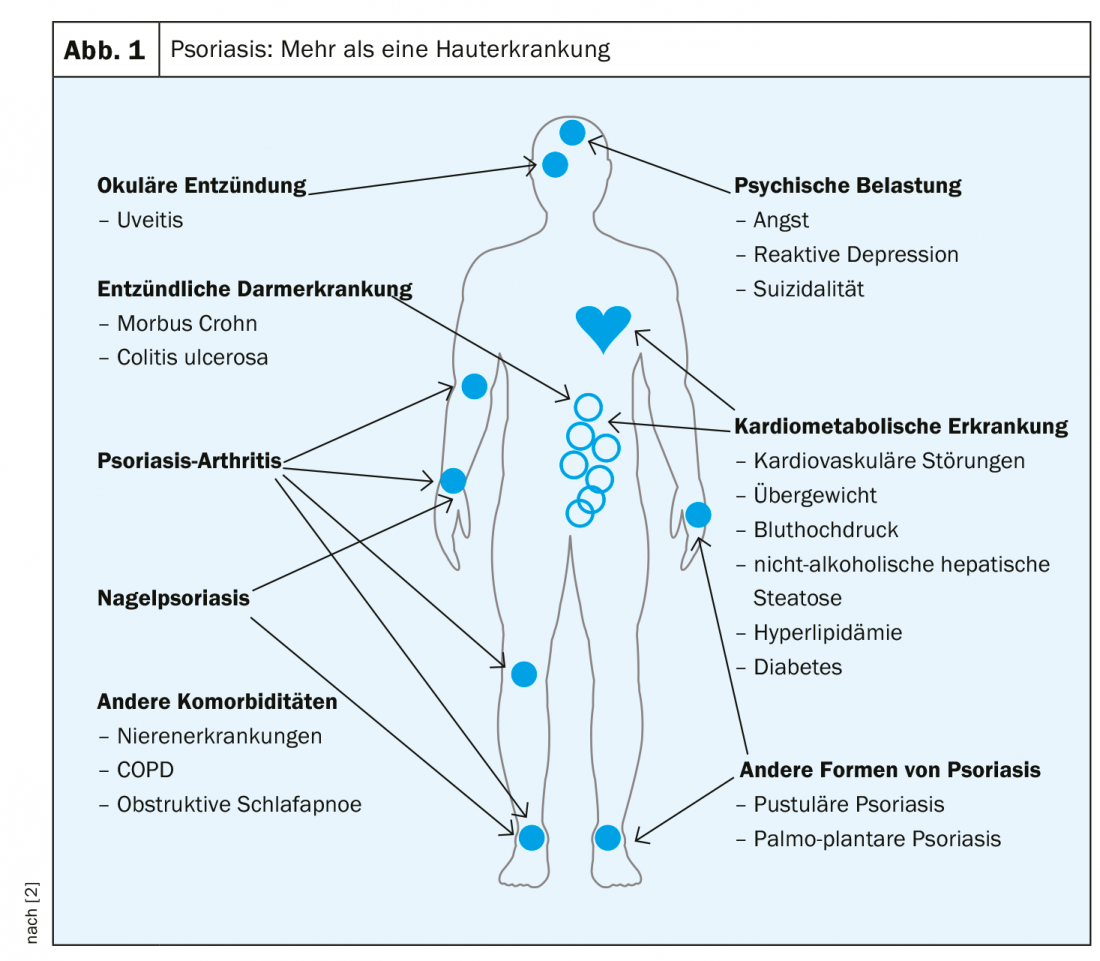
The rate of comorbidity is increased in psoriasis sufferers – about 70% of affected adults have at least one concomitant disease [1]. Psoriatic arthritis occurs in approximately 20% of patients with dermatologically treated psoriasis [1]. There is a significantly increased prevalence of cardiovascular disease, obesity, diabetes, metabolic syndrome, depression, inflammatory autoimmune diseases, and addiction (Fig. 1). Tiago Torres, MD, PhD, University of Porto, presented empirical findings on cardiovascular comorbidities at this year’s EADV Congress [2].
Coronary artery disease, atherosclerotic plaques and the obesity factor
Severe psoriasis not only increases the risk of myocardial infarction and stroke, but also cardiovascular mortality [3]. According to data from a secondary analysis, the prevalence of moderate to severe coronary calcification is fivefold higher in patients with psoriasis than in a healthy control group [4]. In addition, it has been shown that psoriasis sufferers have a similar risk of coronary heart disease as patients 10 years older with hyperlipidemia [2,5]. Cytokine-mediated inflammatory processes implicated in the etiology of psoriasis are thought to be an independent risk factor for cardiovascular comorbidities, which in turn influence the inflammatory mechanisms underlying psoriasis [2]. (Fig. 2). An ultrasound study published in 2019 showed that psoriasis patients have an increased number of arteriosclerotic plaques in the femoral artery compared to a control group and insulin resistance is the most important determinant of atherosclerosis [6]. Obesity is a risk factor for both psoriasis and cardiovascular disease and is associated at the cellular level (proinflammatory cytokines, inflammatory adipokines, anti-inflammatory adipokines) with a state of chronic inflammation [2]. A BMI >30 kg/m2 doubles the risk of psoriasis and the severity of psoriasis is positively correlated with obesity [7]. Adipose tissue is an active endocrine organ that plays an important role in lipid and glucose metabolism and inflammatory processes [7].

Comorbidities must be taken into account
Cardiovascular comorbidities should be considered in the choice of systemic psoriasis therapy, as they may influence efficacy and safety [2]. There is evidence that obesity increases the risk for hepatic and renal toxicity of methotrexate and ciclosporin [7]. In addition, obesity can impair the clinical response of any systemic therapy (conventional and biologics), so a healthy lifestyle and weight loss should be supported [7]. The speaker also drew attention to the fact that some medications used to treat cardiovascular comorbidities may affect psoriasis therapy [2]: Antihypertensives including beta-blockers and ACE inhibitors may worsen psoriasis symptoms in some patients, and interactions between ciclosporins and statins may induce rabdomiolysis. A cohort study demonstrated that improvement in psoriasis severity was associated with a reduction in aortic vascular inflammation at one-year follow-up [8]. And a recent study found that ustekinumab led to significant improvement in aortic inflammatory processes compared with placebo after a 12-week period [9]. A cohort study published in 2019 in patients with moderate to severe psoriasis demonstrated that in biologic-naïve patients (n=89), biologic therapy resulted in a significant reduction in coronary inflammation compared with the conventionally treated control group (n=32) at follow-up one year after baseline [10]. In a retrospective cohort study, TNF inhibitors (TNFi) had a significantly lower risk of major adverse cardiac event (MACE) compared with topical therapy (HR 0.80; 95% CI; 0.66-0.98) [11].
Screening and information are beneficial
According to an international multicenter study published in 2018 (n=2254), there are gaps in diagnosis and care regarding hypertension and dyslipidemia in psoriasis patients [12]. The prevalence of undiagnosed and untreated cardiovascular risk factors in those with severe psoriasis is high [2]. A survey regarding the management of cardiovascular risk factors in patients with severe psoriasis among Portuguese dermatologists found that 45% performed screening/monitoring, but 40% neither clarified cardiovascular risk nor considered it in therapy [13]. An observational study to evaluate the effects of patient education regarding cardiovascular comorbidities showed the following. [14]: before the intervention, the subjects had a low knowledge of appropriate correlations; 6 months after the training, 60.4% increased the frequency of physical activity, 49.1% achieved a weight reduction of 2.3 kg on average, and 50% reduced their nicotine consumption.
Source: EADV, Madrid
Literature:
- Augustin M, et al: Use of system therapeutics and biologics in guideline-based therapy of moderate to severe psoriasis vulgaris. PsoNet Magazine 2017/1.
- Torres T: Treating psoriasis in patients with metabolic comorbidities. Psoriasis treatment, slide presentation, Tiago Torres, MD, PhD, EADV Congress, Madrid, Oct. 12, 2019.
- Armstrong EJ, Harskamp CT, Armstrong AW: Psoriasis and Major Adverse Cardiovascular Events: A Systematic Review and Meta-Analysis of Observational Studies. J Am Heart Assoc 2013; 2(2): e000062.
- Mansouri B, et al: Comparison of Coronary Artery Calcium Scores Between Patients With Psoriasis and Type 2 Diabetes. JAMA Dermatol 2016; 152(11): 1244-1253.
- Lerman JB, et al: Coronary Plaque Characterization in Psoriasis Reveals High-Risk Features That Improve After Treatment in a Prospective Observational Study Circulation 2017; 136(3): 263-276.
- Gonzalez-Cantero A, et al: Subclinical atherosclerosis in psoriasis. Usefulness of femoral artery ultrasound for the diagnosis, and analysis of its relationship with insulin resistance. PLoS One 2019; 14 (2): e0211808.
- Gisondi P, Del Giglio M, Girolomoni G: Considerations for Systemic Treatment of Psoriasis in Obese Patients. Am J Clin Dermatol 2016; 17(6): 609-615.
- Dey AK: Association Between Skin and Aortic Vascular Inflammation in Patients With Psoriasis. A Case-Cohort Study Using Positron Emission Tomography/Computed Tomography. JAMA Cardiol 2017; 2(9).
- Gelfand JM, et al: A Phase IV, Randomized, Double-Blind, Placebo-Controlled Crossover Study of the Effects of Ustekinumab on Vascular Inflammation in Psoriasis (the VIP-U Trial). J Invest Dermatol. 2019 Jul 19. pii: S0022-202X(19)32537-0.
- Elnabawi YA, et al: Association of Biologic Therapy With Coronary Inflammation in Patients With Psoriasis as Assessed by Perivascular Fat Attenuation Index. JAMA Cardiol 2019; 4(9): 885-891.
- Wu JJ, et al: Anti-inflammatory therapy with tumor necrosis factor inhibitors is associated with reduced risk of major adverse cardiovascular events in psoriasis. J Eur Acad Dermatol Venereol 2018; 32(8): 1320-1326.
- Eder L, et al: Gaps in Diagnosis and Treatment of Cardiovascular Risk Factors in Patients with Psoriatic Disease: An International Multicenter Study. The Journal of Rheumatology 2018; 45(3): 378-384.
- Raposo I, et al: Awareness and screening attitudes of Portuguese dermatologists on cardiovascular risk factors in psoriatic patients. Eur J Dermatol 2017; 27(4): 443-445.
- Mota F, Selores M, Torres T: Importance of educational sessions on cardiometabolic comorbidities. Awareness among psoriasis patients. Actas Dermosifiliogr 2016; 107: 539-541.
DERMATOLOGIE PRAXIS 2019; 29(6): 32-33 (published 12/6/19, ahead of print).









