
Regularly administered basic care is an important guideline-based component of treatment, regardless of the severity of atopic dermatitis. In addition to regenerating the disturbed barrier function of the skin, xerosis cutis and itching are reduced. Care should be taken to ensure that the galenic system of the preparation used is adapted to the particular skin condition.
Basic topical skin care is recommended in national and international guidelines for all stages and severities of atopic dermatitis [1–3]. “The basis of all therapy is good basic care with emollients,” explains Prof. Dr. med. Dr. h. c. Andreas Wollenberg. Clinic of the University of Munich [4]. In atopic eczema, a genetically determined lack of or severely weakened immune response to certain antigens causes the epidermal barrier function to be impaired and exogenous factors such as allergens and toxins to penetrate the skin more easily, further weakening the skin barrier and provoking eczema flare-ups. This vicious circle must be counteracted. Adequate basic therapy can prevent an itch-scratch cycle and thus extend the recurrence-free interval. To achieve this, the consistent use of topical preparations for basic care is essential.
Replenishing and hydrating basic care: central for neurodermatitis sufferers
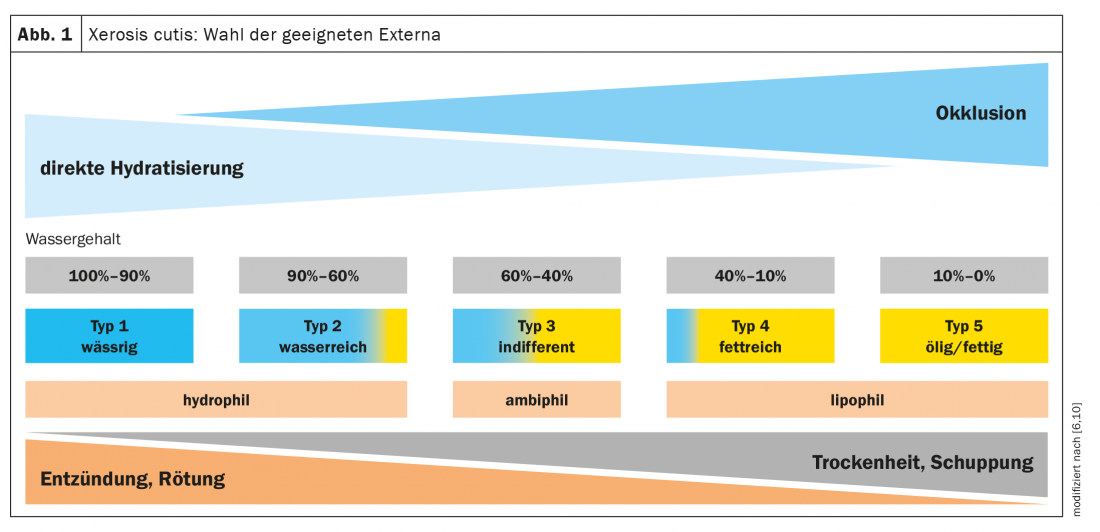
Applying topical basic therapeutics immediately after showering or bathing (“soak-and-seal”) is a very good idea, emphasizes Prof. Wollenberg. The primary goal of basic care is to correct skin barrier disorders that can lead to skin dryness and, as a result, irritation, itching, and spread of the disease-relevant pathogen Staphylococcus aureus [3,5,6]. The galenics of the product used should always be tailored to the individual skin condition, with more hydrophilic formulations being recommended in acute phases of eczema, while more lipid-rich formulations should be used in interval phases [7] (Fig. 1).
Preparations in which hydration-promoting active ingredients are incorporated into the respective base are also known as “humectants”. These are active substances that increase the water-binding capacity of the skin, explains Prof. Wollenberg [8]. In addition to such a hydration-promoting substance as urea, lactic acid or glycerin, an emollient also contains an “occludent” that prevents water loss from the skin, such as petrolatum. In the English-language literature, the terms “moisturizer” and “emollient” are often used in the context of basic care for eczema conditions without a consistent definition of terms, as shown in a Cochrane Review [19].
Externals containing glycerin: well suited for infants
Since glycerin (glycerol) does not cause any skin irritation, the European neurodermatitis guideline recommends glycerin-containing basic care products also for use in infants and young children [3]. Studies have shown that in predisposed infants, early use of such products can reduce the likelihood of developing atopic dermatitis by up to 50% [11,12]. And in a placebo-controlled double-blind study in two- to six-year-old children, improvement in skin dryness lasting for several weeks was shown after only four weeks of application of an O/W cream containing 15% glycerin [13]. Further studies on the hydration-promoting effect of glycerol-containing topicals confirm this finding for use in both children and adults [14–16]. Interestingly, studies have also shown that glycerol-containing topicals in atopic dermatitis can prevent eczema flare-ups and reduce the need for topical glucocorticoids [8,17,18].
In addition to the externals referred to as emollients, which contain no or no pharmacologically active ingredients, the term “emollients plus” has been newly coined in the current European guideline [9]. Examples are preparations with additions of protein-free young oat extract and bacterial lysates from Aquaphilus dolomiae or Vitreoscilla filiformis.
Congress: Update Inflammatory Skin Diseases
Literature:
- Eichenfield LF, et al: J Am Acad Dermatol 2014; 71: 116-132.
- Werfel T, et al: JDDG 2016; 14: 92-106.
- Wollenberg A, et al: J Eur Acad Dermatol Venereol 2018; 32: 657-682.
- Wollenberg A: Update atopic eczema. 5th Lübeck Update: Inflammatory Skin Diseases, 05.03.2022
- Werfel T, et al: Guideline Neurodermatitis [atopic eczema; atopic dermatitis]. As of 03/31/2015. www.awmf.org, (last accessed 03/08/2022).
- Augustin M, et al: Position paper – Diagnostics and therapy of xerosis cutis. JDDG 2018 (16), Suppl 4, 3-35.
- Statement of the Gesellschaft für Dermopharmazie e. V. Topical basic therapy for neurodermatitis,
- www.gd-online.de (last call 08.03.2022)
- Rossi AB, et al: Dermatol The(Heidelb) 2018; 8: 217-228.
- Wollenberg A, et al: Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. J Eur Acad Dermatol Venereol 2018; 32: 657-682.
- Wohlrab J, et al: S2k guideline on the use of preparations for topical application to the skin (topicals). Status: 01.11.2017. www.awmf.org
- Simpson EL, et al: J Allergy Clin Immunol 2014; 134: 818-823.
- Horimukai K, et al: J Allergy Clin Immunol 2014; 134: 824-830.
- Boralevi F, et al: J Eur Acad Dermatol Venereol 2014; 28: 1456-1462.
- Blanchet-Bardon C, et al: J Eur Acad Dermatol Venereol 2012; 26: 1014-1019.
- Lodén M, et al: Acta Derm Venereol 2002; 82(14): 45-47.
- Cristaudo A, et al: G Ital Dermatol Venereol 2015; 150: 297-302.
- Tiplica GS, et al: Pediatr Dermatol 2017; 34: 282-289.
- Tiplica GS, et al: J Eur Acad Dermatol Venereol 2018; 32: 1180-1187.
- Van Zuuren EJ, et al: Cochrane Database of Systematic Reviews 2017; 2: Art.No CD012110.
DERMATOLOGIE PRAXIS 2022; 32(2): 26-27









