CT-guided PRT has become a recognized minimally invasive spine pain management procedure. It is an efficient, low-risk procedure with few side effects that can be performed on an outpatient basis. With an average of 3 to 5 treatments at approximately three-week intervals, a long-lasting relevant reduction in pain or freedom from pain can be achieved in about 80% of patients.
Musculoskeletal disorders are among the health problems that place the greatest economic burden on the economies of developed countries. Obesity and physical inactivity lead to significant degenerative changes in the musculoskeletal system with pain syndromes. 25% of cases are of chronic progressive course. Women are affected more often than men. In the sixth and seventh decades of life, a gradual decrease in the frequency of disease is observed.
Currently, there is an increasing shift of spine-related pain to younger and younger cohorts. Already at the age of 10 to 17 years, about 70% of children and adolescents complain about problems of the trunk skeleton that interfere with everyday life.
Following the article on disc extrusion with radicular symptoms, today we will refer to the possibility of minimally invasive CT-guided periradicular therapy (CT-PRT).
In acute radicular pain, after about 6 to a maximum of 8 weeks of conservative, multimodal therapy with medicinal, physical and physiotherapeutic measures, the indication for minimally invasive treatment is given if there is no contraindication. The clinical symptoms must correlate with the findings on cross-sectional imaging.
The therapeutic goal of all treatment measures is to reduce pain until patients are pain-free, enabling them to return fully or at least partially to their normal daily lives, occupations and social activities. Radiologically controlled minimally invasive therapies have established modalities that are low-risk, effective, persistently analgesic, and can be considered significantly less costly compared with prolonged conservative measures or inpatient treatments. Already about 25 years ago, it was recognized that surgical interventions could thus be avoided in many cases. Meanwhile, various studies support these statements that long-lasting pain reduction can be achieved with a complication rate of CT-PRT below 1%. Up to 95% of patients benefited with significant pain reduction over a mean of 9 months.
Legal aspects have become increasingly important, especially in the case of interventional measures. Even if the therapy is technically flawless and there are no complications, there may be legal consequences if the patient has not been properly informed about the treatment. Overview 1 provides information on the most important aspects.
Clarifications: what to consider
- Education must be provided in a timely manner; the circumstances of an emergency with education provided immediately prior to the procedure cannot be invoked for periradicular therapy as an elective treatment
- comprehensive information about the implementation, specific risks, possible consequences and alternatives of the therapy
- prefabricated patient information sheets can facilitate the information, but do not replace the personal information by the treating physician; in case of delegation to a medical colleague, it must be ensured that the information meets the requirements; delegation of the information to the MTAR or medical assistant is not permitted. Individual aspects of the information must be documented in the case of standardized information sheets and signed by the physician providing the information and the patient after the information has been provided. In this context, the patient must be capable of grasping the significance and consequences of his or her decision, which requires neither capacity under civil law nor criminal culpability, but capacity for insight and judgment in the “natural sense”.
- the following applies: the information must be provided in good time, comprehensively, individually and in a comprehensible manner.
The information may be omitted if the patient states emphatically and in writing that no information is desired.
The classic indications for CT-guided PRT have not changed over the years, listed in Table 2.
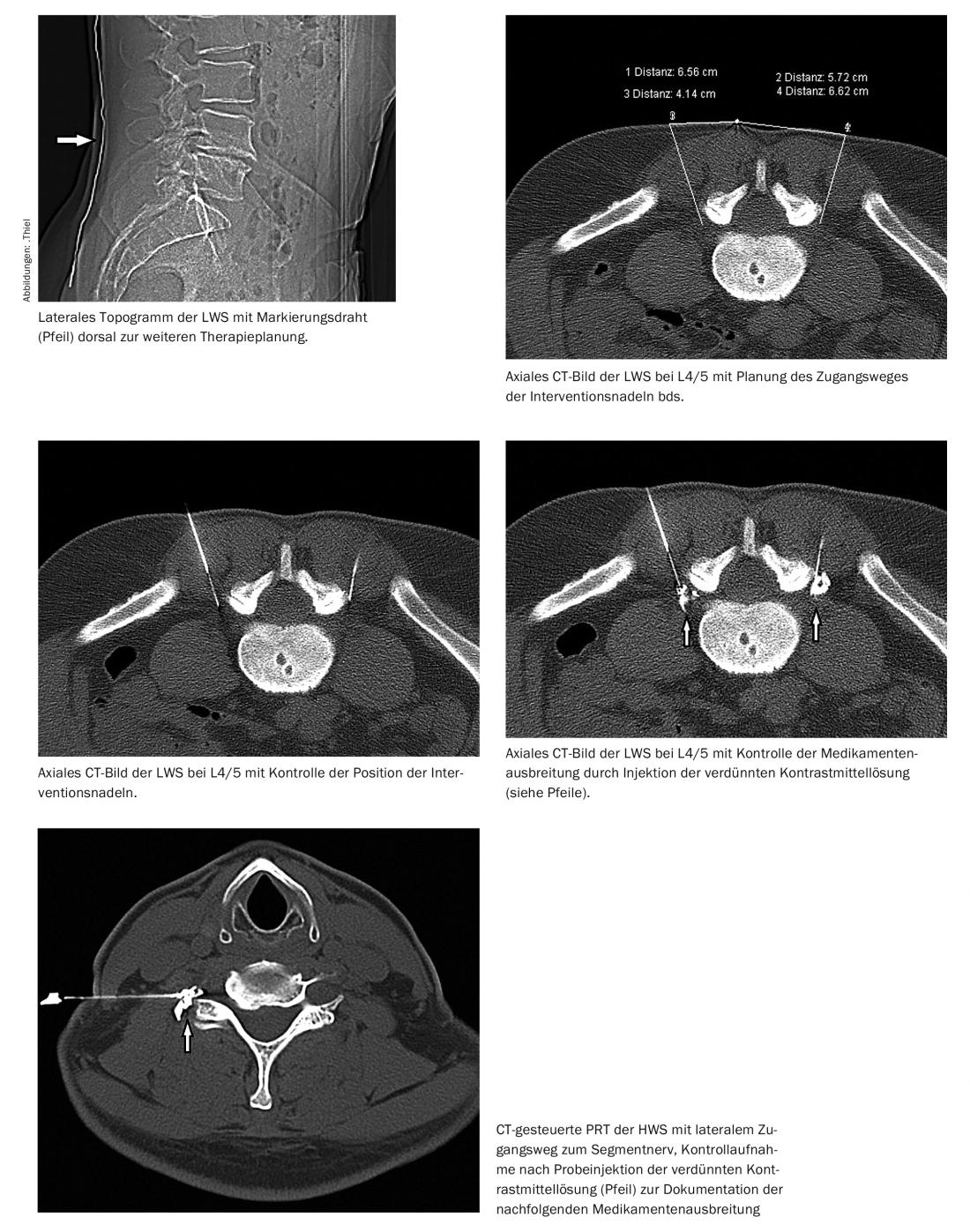
The technique, which goes back to Macnab, and the course of treatment also represent standardized procedures.
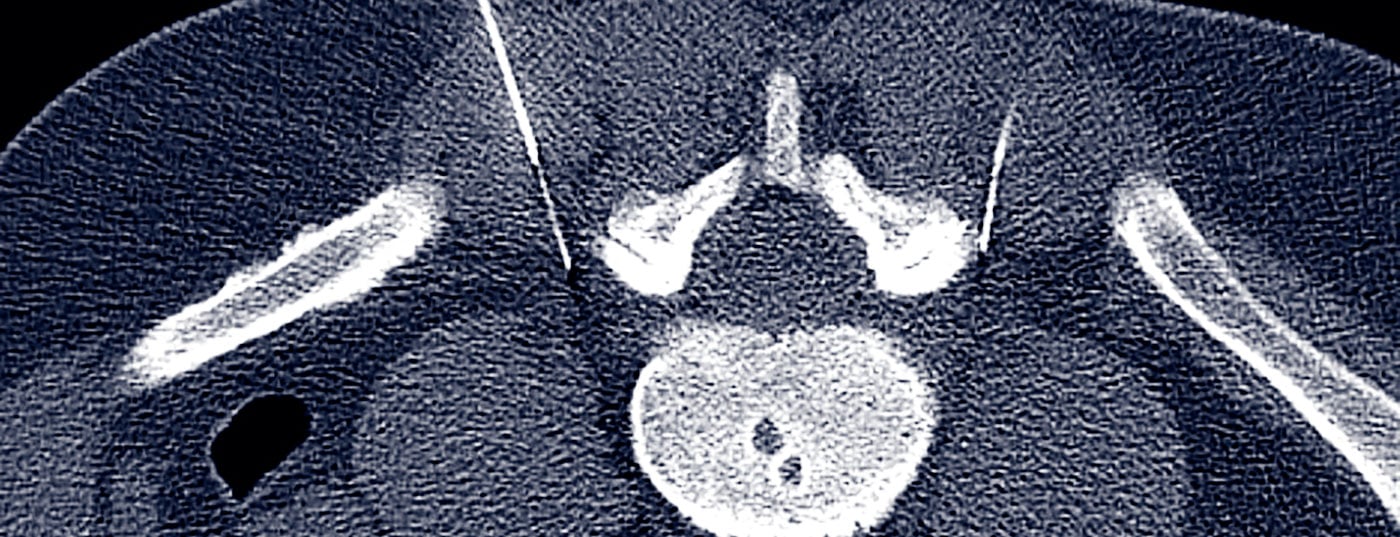
CT-guided vertebral nerve root treatment, can be performed as a periradicular extraspinal injection technique or as an intraspinal epidural drug application. The treatment can be performed without a guide needle for short distances from the skin surface to the nerve, and with a guide needle for longer distances, i.e. using the coaxial technique. This problem occasionally has to be faced during CT-PRT of obese patients also at the cervical spine.
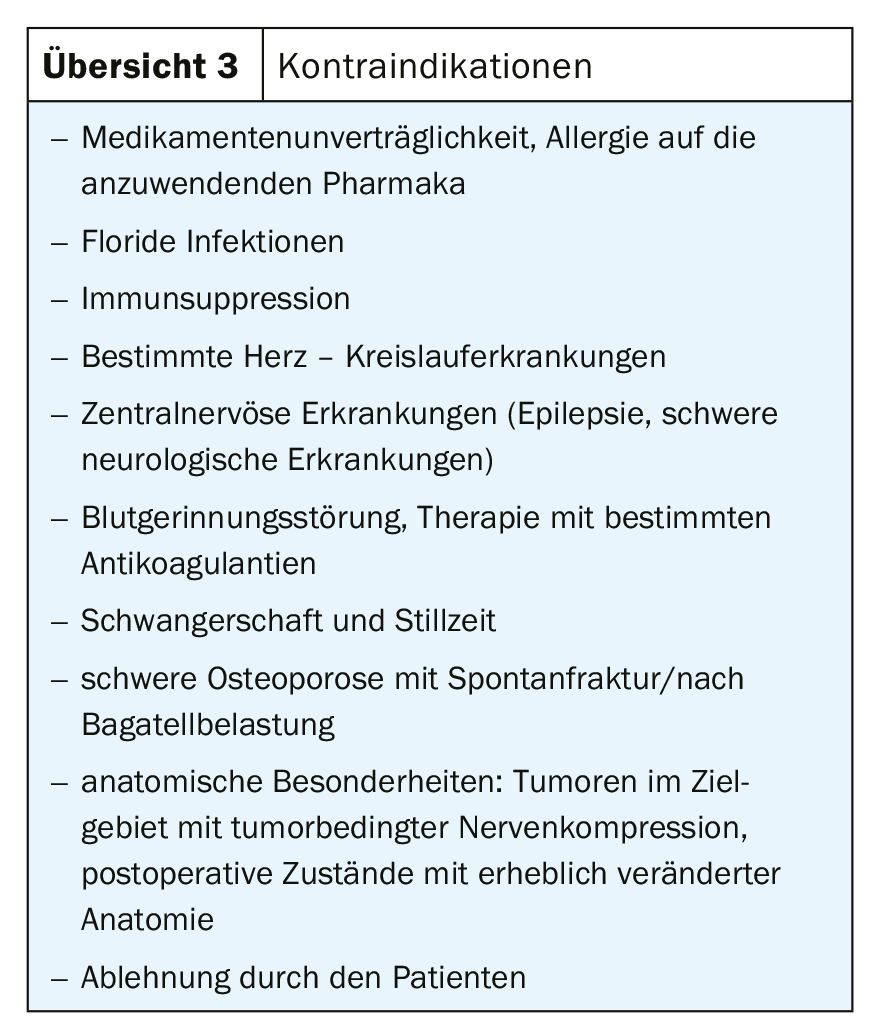
The contraindications of the therapy are summarized in overview 3, the detailed description can be found in the given literature.
Further reading:
- Grönemeyer DHW, Thiel HJ, Moser C: Tomographic periradicular microtherapy. ABW Wissenschaftsverlag GmbH, Berlin; 2013.
- Thiel HJ: CT-guided PRT for MTRA. ABW Wissenschaftsverlag GmbH, Berlin; 2014.
- aerzteblatt.de, 13.11.2013
- Thiel HJ: CT-guided periradicular therapy – updates on planning and implementation. radiology technology 1/2018: 4-7.
HAUSARZT PRAXIS 2019; 14(12): 25-27









