Transsexuality, tansgender, transidentity are terms that have been read and heard more and more often in recent months. Until recently, was declared a mental disorder, but a more (self-)understandable approach is now being sought. This perception of people’s gender as not purely binary allows for a range of gender identities and requires a new way of thinking.
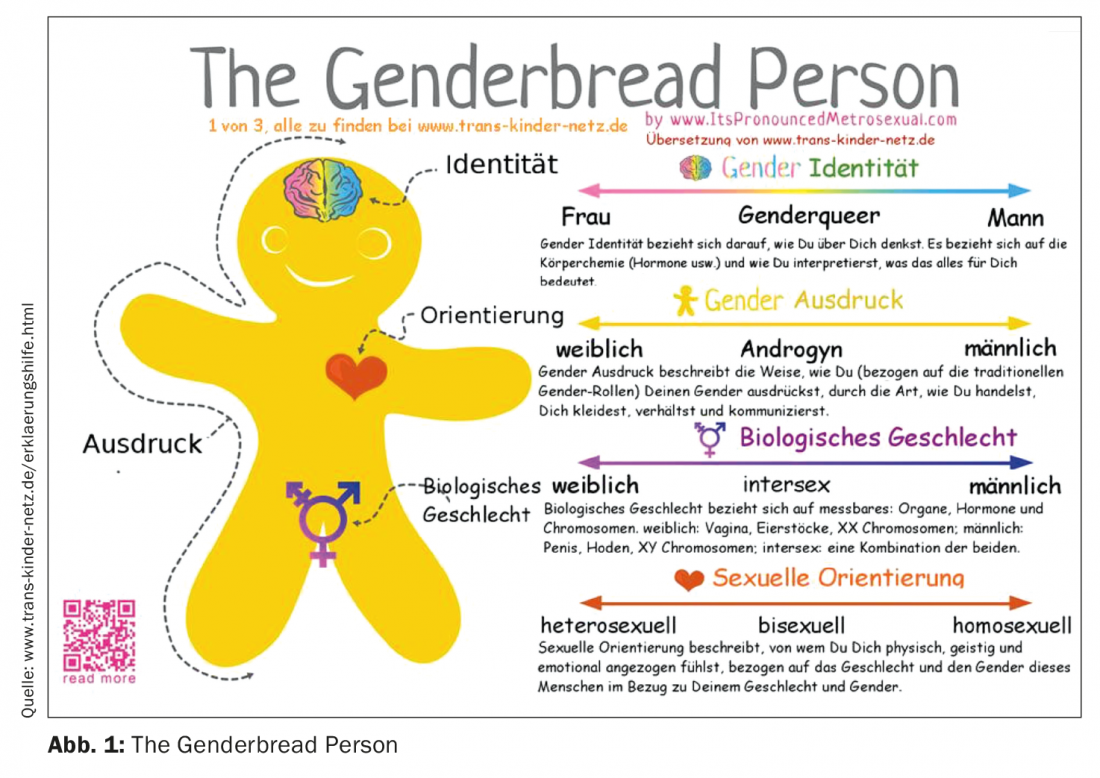
Until the turn of the millennium, the term “trans” was still used rather disparagingly and pejoratively for people whose gender affiliation could not be clearly assigned. Fortunately, a lot has changed in the meantime. Nevertheless, it is still not easy to keep track and to assign the many new impressions and designations. Basically, a distinction must be made between gender identity and sexual orientation. One describes who you are, the other who you love, as Dr. med. Rahul Gupta, Graubünden, put it in a nutshell. It can be represented in an even more differentiated way if one distinguishes between identity, orientation, expression and biological sex (Fig. 1) .
In a Dutch online survey with 8064 participants, 4.6% of men and 3.2% of women described themselves as ambivalent and/or incongruent toward their own gender. This corresponds to a prevalence of 1.1% and 0.8%, respectively. In a Belgian study, the prevalences were 2.2% and 1.9%, respectively.
www.trans-kinder-netz.de/erklaerungshilfe.html
Guidelines and their handling of transsexuality
Still in the ICD-10 transsexualism was classified as a disorder of gender identity and therefore declared as a mental disorder. In the subsequent classification, which is to come into force at the beginning of 2022, this aspect has been revised. The term “gender incongruence” is intended to express the incongruence between gender and gender of assignment and replaces the previous terminology. The Diagnostic and Statistical Manual of Mental Disorders (DSM), in its 4th edition, introduced the term “gender identity disorder” in place of “transsexualism” and placed it in the category of “sexual and gender identity disorders.” The DSM-5 eventually replaced the term “gender identity disorder” with “gender dysphoria” and no longer considers trans identity itself a mental disorder, but rather the condition created by the incongruence between biological sex and gender identity. This represents an important step toward de-pathologization, with no risk that health insurance would no longer provide benefits. A balancing act that tries to do justice to all aspects. Already in 2002 it was demanded that psychiatry should distance itself from the pathological concept of transsexualism and regard it as a norm variant.
The S3 guideline Gender Incongruence, Gender Dysphoria, and Trans Health points out that limited access to the health care system, stigma, and discrimination are associated with significant health risks. Therefore, those seeking treatment should be guaranteed unrestricted access to health care. This also includes psychosocial support, counseling and, if necessary, psychotherapy in order to be able to cope with and deal with the consequences of trans negativity and trans hostility and to prevent secondary mental disorders.
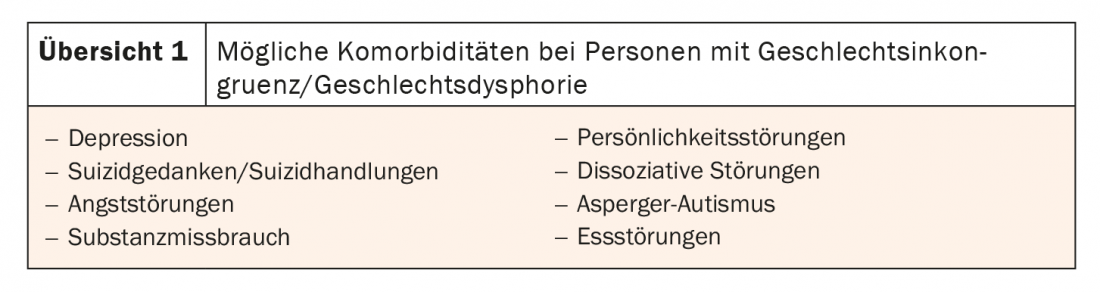
The diagnosis should also cover psychological, physical, social and cultural aspects and result in a holistic view of the person seeking treatment. The history should record whether the gender incongruence and/or gender dysphoria has been constant for at least a few months, is transient, or intermittent. Also, comorbidities should not be disregarded, which have been shown to have increased prevalence rates in clinical trials (review 1).
Congress:
FomF Update Refresher
InFo NEUROLOGY & PSYCHIATRY 2021; 19(4): 21 (published 8/20-21, ahead of print).