Current European guidelines advocate strict LDL-C lowering to prevent cardiovascular disease. Statins, which can significantly lower both total and LDL cholesterol, play a central role. In addition, PCSK9 inhibitors achieve effective results, especially in statin intolerance. Is lipid apheresis still needed at all?
The causal role that LDL cholesterol plays in the development of atherosclerosis is now undisputed. Elevated cholesterol is considered a major risk factor for the development of atherosclerosis, which also increases the risk of cardiovascular events [1]. Studies have demonstrated that the incidence of cardiovascular events decreases with the reduction of LDL cholesterol levels [2].
Dyslipidemia is characterized by an elevated plasma cholesterol and/or triglyceride (TG) concentration or a low HDL level in the blood. In primary dyslipidemia, there is a genetic predisposition. Secondary dyslipidemia can be triggered by, among other things, a sedentary lifestyle, excessive intake of saturated fatty acids, cholesterol, and trans fats, diabetes mellitus, hypothyroidism, or medications (especially beta-blockers, thiazide diuretics, cyclosporine, tacrolimus, estrogens, glucocorticoids).
Optimized treatment management
Lifestyle modifications, such as a switch to a healthy diet and more active lifestyle, rarely lead to success on their own. Since atherosclerosis is an inflammatory process, it is obvious to use anti-inflammatory and antioxidant drugs for vascular prevention. Statins are considered the drug of choice. Their lipid-lowering effect occurs via inhibition of HMG-CoA reductase, the key enzyme in cholesterol biosynthesis. This inhibition results in decreased formation of LDL cholesterol with concomitant increased expression of hepatic LDL receptors [3]. However, optimal treatment of dyslipidemia is still far from being achieved. One study demonstrated that less than 16% of CHD patients achieved the LDL cholesterol target of <1.4 mmol/l despite effective lipid-lowering therapy [4].
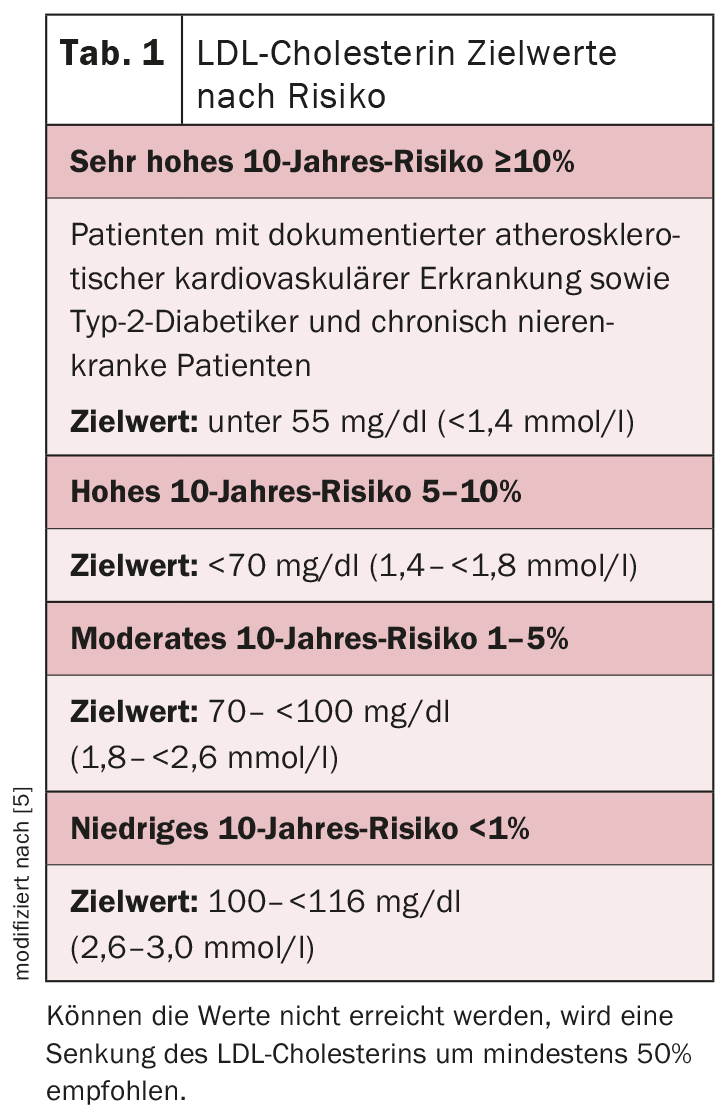
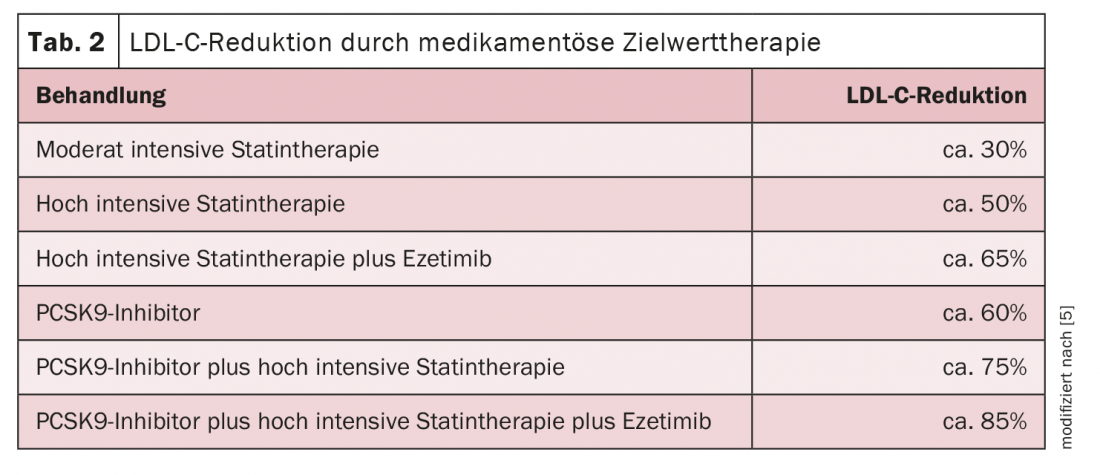
The LDL-C target value is based on the patient’s determined risk (tab. 1). To achieve the individual risk level, high-potency statins up to the highest tolerated dose should be used in the first instance. If the target values are not reached by the use of a statin, a combination of statin and ezetimibe is recommended. If this treatment regimen is still not sufficient in the case of high or very high risk, the further addition of a PCSK9 inhibitor is conceivable (Table 2) [5]. With this, a proven effective lipid reduction of up to 60% can be achieved. The monoclonal antibody binds to the protein PCSK9, preventing it from docking to the LDL receptors. This increases the uptake of LDL cholesterol from the blood into the liver. In addition to patients with a very high cardiovascular risk and heterozygous familial hypercholesterolemia, the new substance class can currently be used primarily in patients with statin intolerance.
End of the line: lipid apheresis
In patients with LDL cholesterol elevation >130 mg/dl and/or Lp(a) elevations >120 nmol/l (approx. 60 mg/dl), the performance of lipoprotein apheresis should be discussed in case of clinically or imaging proven progression of vascular disease. In addition, it should be considered for:
- Patients with homozygous familial hypercholesterolemia.
- Patients with severe hypercholesterolemia in whom diet and medications do not adequately lower LDL cholesterol over a documented 12-month period.
- Patients with isolated Lp(a) elevation and documented progressive cardiovascular disease (e.g., coronary artery disease, stroke, atherosclerosis of the brain-supplying vessels, or peripheral arterial disease).
Under regular apheresis – usually once a week – LDL cholesterol reductions of up to 80% can be achieved.
Literature:
- Ference BA, Ginsburg HN, Graham I, et al: Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. evidencefromgenetic, epidemiologic, andclinicalstudies. A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur Heart J 2017; 38: 2459-2472.
- Boekholdt SM, HovinghGK, Mora S, et al: Very low levels of atherogenic lipoproteins and the risk for cardiovascular events: a meta-analysis of statin trials. J Am Coll Cardiol 2014; 64: 485-494.
- www.amboss.com/de/wissen/Lipidsenker (last accessed on 24.08.2021)
- Guha M, Völler H, Eckrich K et al: The current ESC LDL-C target <1.4 mmol/l is achieved in less than 16% of patients with CHD despite effective lipid-lowering therapy: data from the LLT registry. Clin Res Cardiol 109, Suppl 1, April 2020 – Article V1796.
- Mach F, Baigent C, Catapano AL, et al: 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J 2020; 41(1): 111-188.
CARDIOVASC 2021; 20(4): 24-25









