
Breaches in care between the ambulatory and inpatient care sectors have various implications for all parties involved in the care process. As part of a study project in Germany, a patient-oriented referral and discharge management system was implemented and evaluated in primary care practices and hospitals.
Care management concerns the processes and actions of care at the level of medical institutions [1]. Breaks in care between outpatient and inpatient settings jeopardize the care process, reduce patient satisfaction, and are associated with avoidable health economic costs [2]. The goal of the VESPEERA project (“Securing continuity of care – patient-oriented referral and discharge management in GP practices and hospitals”) was to establish communication structures between hospitals, GP practices and health insurance in order to optimize cross-sector care in referral and discharge management. The project was implemented in the period 2017-2020. The client was the German Innovation Committee at the Federal Joint Committee [3].
Structural referral and discharge management offers several advantages
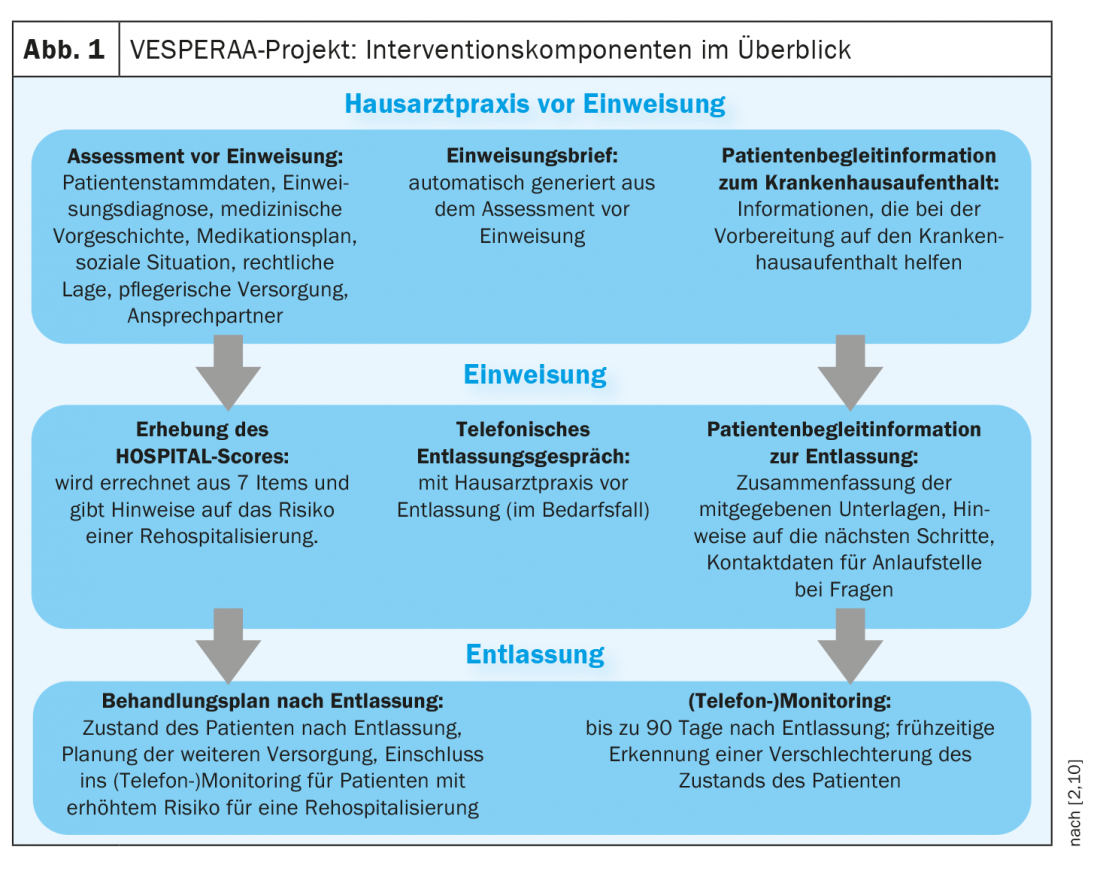
Admission and discharge management according to the VESPEERA concept (Fig. 1) can lead to lower rehospitalization rates and shortens the length of hospital stay for older patients, according to a conclusion of the project team [2,4,5]. Potential target groups are especially elderly patients respectively patients with high comorbidity and with increased risk for rehospitalization in general. In this context, admission and discharge management should not be reduced to the timing of admission and discharge. In summary, structural referral and discharge management offers numerous labor and cost economic benefits [2,4,5].
Information and communication flow as an important factor
The VESPEERA project showed that patients are often discharged from inpatient settings with too little preparation. If relatives or continuing care physicians are not adequately informed, this can have a negative impact on the design of continuing care [2,6]. From the patient’s perspective, there are certain deficits in the area of coordination between the outpatient and inpatient sectors and in the flow of information and communication [7]. Also addressed as a potential problem area are different cultures and goals of care between hospitals and practices or in interprofessional teams [8,9].
Very important: Networking between primary care physician and inpatient facility
One of the conclusions in the evaluation report is that the primary care physician should already be informed during the inpatient stay if a need for complex, seamless follow-up treatment becomes apparent [2]. It is proposed to define exchange formats or interfaces for this purpose that enable time-independent communication between hospital and physician practice. The provision of more information by established physicians at referral should be encouraged. Another finding is that primary care physicians should be more involved in follow-up care. Ideally, referral and discharge management is viewed as a shared cross-sector responsibility. Risk assessment (e.g., using the HOSPITAL score) at hospital admission and at discharge can identify a risk for unplanned readmissions in a timely manner [2]. It is also recommended to determine which communication channel is suitable for which information. Moreover, it would be desirable if patients were more involved in the process of sector transition, informed about it and clarified, according to another conclusion of the VESPERAA project.
Literature:
- Wendt WR: Care and case management, In: Otto H-U & Thiersch H (eds) (2011): Handbuch Soziale Arbeit, 4th completely revised edition, Munich: Ernst Reinhardt Verlag, p. 214.
- Forstner, et al: VESPERAA: Admission and Discharge Management, Attachment No. 5: Evaluation Report, https://innovationsfonds.g-ba.de, (last accessed 09/09/2022).
- “Gesundheitsoekonomie”, www.aqua-institut.de/wissenschaft-forschung/gesundheitsoekonomie, (last accessed 09.09.2022).
- Gonçalves-Bradley DC, et al: Discharge planning from hospital. Cochrane Database Syst Rev; 2016:CD000313.
- Jenq GY, et al: JAMA Intern Med 2016: 176: 681-690.
- Hesselink G, et al: BMJ Quality & Safety 2012: 21 Suppl 1: i39-49.
- Ludt S, et al: Public Health 2014: 76: 359-365.
- Sampson R, Barbour R, Wilson P: BMC Fam Pract 2016: 17: 45.
- Goldman J, et al: Journal of Interprofessional Care 2016: 30: 217-225.
- Forstner J, et al: Ensuring continuity of care: patient-oriented referral and discharge management in family practices and hospitals (VESPEERA). Düsseldorf: German Medical Science GMS Publishing House; 2019.
HAUSARZT PRAXIS 2022; 17(9): 34
InFo PNEUMOLOGY & ALLERGOLOGY 2022; 4(4): 30









