
It wasn’t enough to win the World Cup, but the enthusiasm of the Swiss during the World Cup clearly showed the importance of the king of sports. National sports injury statistics also demonstrate this preference, with football injuries accounting for nearly a quarter (24%) of all national sports injuries. Injured football players are therefore something commonplace in family practice.
Accident insurance (SSUV) statistics show which parts of the body are most often affected when kicking: Lower legs, ankles and feet (40%), knees (18%), wrists and hands (11%) and torso and back (6.7%). The type of injury consists mostly of sprains and strains (36.2%), followed by superficial injuries and contusions (24.5%), and muscle and tendon injuries (13.9%).
Professional footballer: a high-risk profession
The accident statistics for professional footballers are somewhat different. A survey conducted exclusively in top-level football at European level (UEFA, Champions League clubs over 12 years) shows that muscle injuries are the biggest risk for professionals. Muscle injuries are often underestimated in “normal” medicine, although they can cause very long absences in competitive sports (six to eight weeks). Shaquiri and Barnetta can tell you a thing or two about it! An even more detailed analysis of the UEFA survey also reveals something worrying: the injury rate in professional football is almost 1,000 times higher than in high-risk activities in the industry. It should be mentioned here that in our country these football “workers” are also UVG insured.
The “Football ankle
Football is played mainly with the feet, so when injuries occur, the feet and ankles are often affected. In addition to the “classic” ankle distortion, there are other disorders specific to soccer, which can even be found in the literature under the term “football ankle” or “soccer ankle” (respectively anterior and posterior impingement syndrome).
- In the ventral form, tibiotalar osteophytes develop in response to the myriad microtrauma and are responsible for the symptoms. The diagnosis is clinical, and the radiograph is normal. Treatment initially consists of rest, but (arthroscopic) ablation is often necessary.
- The dorsal form involves the processus posterior tali and/or an os trigonum. Repeated plantar flexions, i.e. every time you kick a soccer ball, cause irritation and consequently pain in the area. Again, the diagnosis is clinical – brusque manual plantar flexion by the physician triggers the pain. A lateral x-ray, or at most an MRI or scintigraphy, will confirm the diagnosis. Therapy consists of taping to restrict plantar flexion through infiltrations to surgical revision. Experience shows that it takes at least two months before sporting activities can be fully resumed.
Groin strain
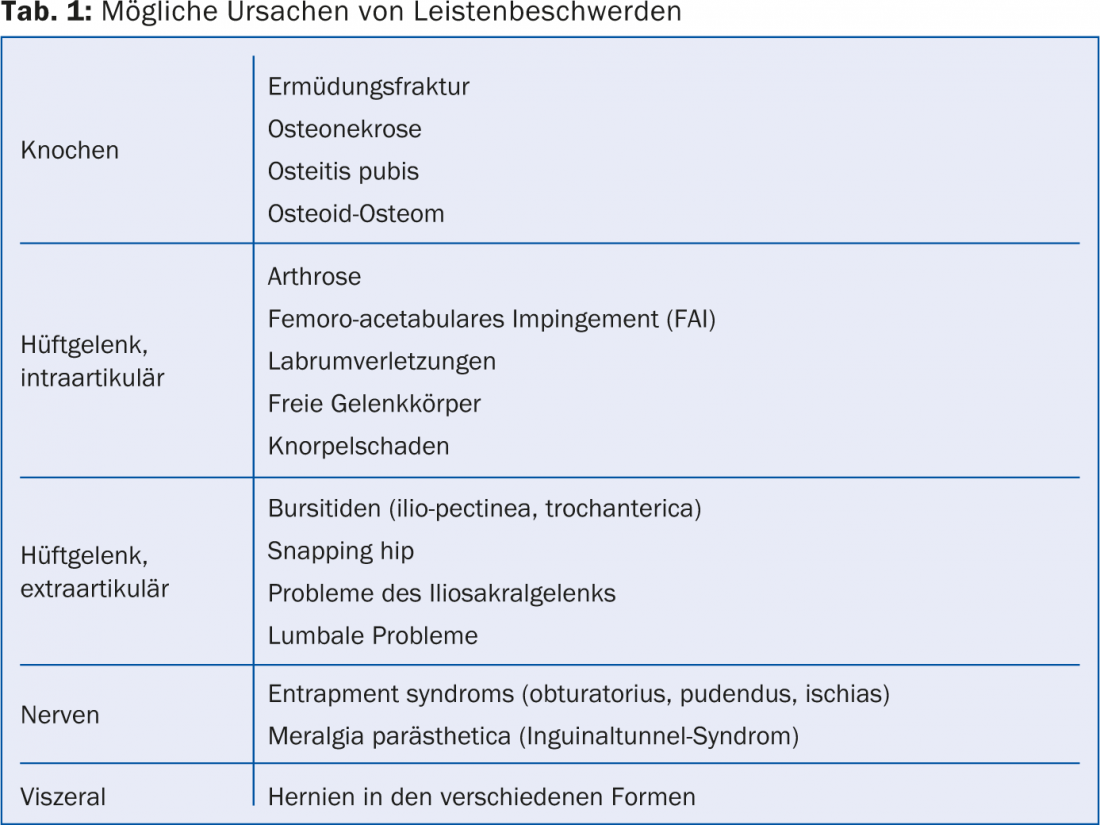
Another almost football-exclusive health disorder is the so-called groin strain. An acute groin strain is most commonly caused by a muscle fiber tear of the adductor muscles, and in adolescents also by an osseous avulsion at the pelvis at the base of one of the powerful knee extensors. Much more common, however, are insidious symptoms of overuse of the groin (pubalgia), which are quite difficult to diagnose accurately. It is a real challenge for the treating physician to find the correct cause of groin pain, because the list of differential diagnoses is long (Table 1). It is therefore important to have a good idea of the local (complex) anatomy, to take a very careful history, to perform a meticulous examination and to use targeted ancillary examinations (X-ray, MRI, sonography). Often the course is extremely difficult and the complaints improve only slowly.
Muscle fiber tears
Muscle fiber tears are easy to diagnose – the athlete often does it himself – but prevention, fine diagnostics and therapy are quite difficult. Stretching has no proven effect, and so far no risk factors for such a lesion have been found. Sonography helps well to define the extent of the tear and to estimate its course. It is optimal if the attending physician can make this clarification himself. In therapy, surgical intervention is rarely necessary. Whether physiotherapeutic measures or PRP injections (centrifuged autologous blood with a high content of growth factors from platelets) really work has not been conclusively proven scientifically. However, the regeneration tendency of the muscles is six to eight weeks. During this time, substitute training is essential.
FIFA: a model association in terms of sports medicine
Finally, a remark: FIFA is often criticized quite heavily, but in terms of sports medicine it is the model association par excellence. It provides human and financial resources to support football-specific research. This results in practically relevant outcomes (e.g., changes to the rules of the game) that benefit other sports as well.
HAUSARZT PRAXIS 2014; 9 (9): 7-8









