
Hearing loss often goes unnoticed or uncompensated for a long time, but affects the lives of those affected in many ways. It is useful to systematically include questions about hearing and speech comprehension in the case history, especially in older patients. Personal motivation and realistic expectations are crucial for successful fitting of a hearing aid, because fitting a hearing aid takes time, patience and perseverance. Today, a wide range of hearing aids is available so that most hearing losses can be satisfactorily treated.
It can be assumed that primary care physicians are confronted with hearing loss in their daily practice. In most cases, however, the hearing loss is not the reason for or the subject of the consultation, but is conspicuous by communication problems in conversation.
As an excellent connoisseur of his patients, the family doctor is the first point of contact for hearing disorders and communication problems. This article provides up-to-date knowledge about the process and possibilities of hearing aid provision in Switzerland, as a basis for optimal counseling of affected persons.
What are the effects of hearing loss?
With hearing loss, life becomes more complicated. Speech intelligibility is quickly impaired, leading to comprehension problems, especially in background noise and group conversations. Increased listening effort, easier fatigue and irritability, social withdrawal and avoidance of social occasions are the consequences [1].
Associations between hearing loss and decline in cognitive abilities [2,3] as well as hearing loss and concentration problems and decline in performance at work are also known [4]. The interaction between dementia and (un)attended hearing impairment is currently being investigated by several research groups.
How can hearing loss be detected?
Hearing loss often goes unnoticed for a long time because the changes are slowly progressive and the affected individuals automatically adapt their behavior to the situation by placing themselves on the sidelines in company or avoiding difficult listening situations. It is not uncommon for those affected to be first approached by those around them about a possible hearing loss.
Increasing tinnitus or sensitivity to noise, as well as concentration problems and a drop in performance, can indicate hearing loss. We therefore recommend that questions about hearing and speech comprehension be systematically included in the case history.
How to proceed with hearing loss?
A rough evaluation of the hearing is easily possible in practice. The tuning fork test according to Weber and Rinne can be used to distinguish a sound transmission disorder from a sound perception disorder. However, the tuning fork is not suitable for more advanced hearing testing because only one frequency (440 Hz) is tested. Otoscopy is essential to detect ear canal, tympanic membrane, and middle ear pathologies. With the auditory range test or the whispering number test, speech comprehension can be roughly estimated at rest.
The self-tests of hearing that are widely available on the Internet (e.g. pro audito Telefonhörcheck, Tel. 0900 400 555, Fr. 0.50/min.) can provide indications of a hearing disorder, but are no substitute for an audio audiogram by a specialist. Often only four frequencies are measured in the self-tests, the measurement conditions are not standardized, masking of the opposite ear is not possible and thus no side-separated measurement is guaranteed. It is also not possible to measure the bone conduction hearing threshold. When patients with hearing impairment take such a test and it comes out “normal”, they are confused and look elsewhere for the reasons for their problems.
If a hearing disorder is suspected, an ENT specialist examination with sound audiogram using calibrated equipment in a listening booth (air and bone conduction from 0.25-8 [12] kHz) and speech audiogram at rest and in noise is recommended. The speech audiogram better reflects communication problems in everyday life than the tone audiogram. Subjective impairment (hearing handicap) is best assessed using standardized questionnaires, for example, the HHIE-S (Hearing Handicap Inventory-Screening: www.uspreventiveservicestaskforce.org/Home/GetFileByID/231) [5].
Who needs a hearing aid?
Although increasing hearing loss with age is common and communication technology is ubiquitous with smartphones, headphones and accessories, hearing aids are still perceived as a stigma and rejected by many affected individuals. That is a pity! Well-functioning hearing makes daily life easier, helps with orientation, warns of danger and conveys enjoyment in conversation and music.
The answer to the question of when a hearing aid is indicated depends not only on the degree of hearing impairment, but above all on individual hearing requirements and the acoustic and communicative demands of everyday life. If a hearing disorder and a corresponding hearing handicap exist, the affected persons should first be advised by the ear specialist about hearing-improving measures. In addition to conventional hearing aids, hearing enhancement surgery or an implantable hearing aid may be an alternative.
Personal motivation to improve hearing with a hearing aid and realistic expectations are critical to successful care. The type of fitting recommendation is also based on individual hearing requirements and demands. There are no age limits. We urgently recommend a fitting if the hearing loss poses a risk at the workplace or for people in training.
Hearing aid fitting procedure and financing
Hearing aids belong to the aids and are supported by the IV/AHV with a voluntary cost contribution (registration at www.ahv-iv.info, search term “hearing aids”). The goal is a simple and expedient supply. If there were or are potentially hearing-damaging influences at the workplace (noise) and a hearing loss compatible with this, a registration with SUVA should be considered. The patient must therefore register for cost sharing with the insurer himself using the appropriate form (IV/AHV or SUVA). Proper education already in the family practice and at the ear specialist helps the patient to make the right choice regarding a hearing aid and to avoid hasty hearing aid purchases directly from the provider. The ENT physician receives the order from the insurer for the hearing aid expertise, consisting of consultation and sound and speech audiogram. From the audiograms, the total hearing loss per ear is calculated as a percentage. If the threshold value is reached (20% hearing loss for IV, 35% for AHV), the insurer pays a lump sum towards the purchase of hearing aids, regardless of the type and extent of the hearing impairment and the professional and personal requirements for a hearing aid (Tab.1). Detailed information on the hearing aid fitting process, with instructions for patients, can be found at www.luks.ch/standorte/luzern/kliniken/hals-nasen-ohrenklinik/medizinisches-angebot/ohr/hoergeraeteversorgung.html.
From an ENT physician’s point of view, we recommend aiming for an optimal fitting of both ears with maximum possible hearing gain, regardless of cost sharing by the insurer. I don’t think it would occur to anyone to buy glasses that make you see just a little better, rather than glasses that normalize your visual acuity. Binaural fitting and modern signal processing contribute to successful hearing aid fitting [6].
Which hearing aid for which hearing loss?
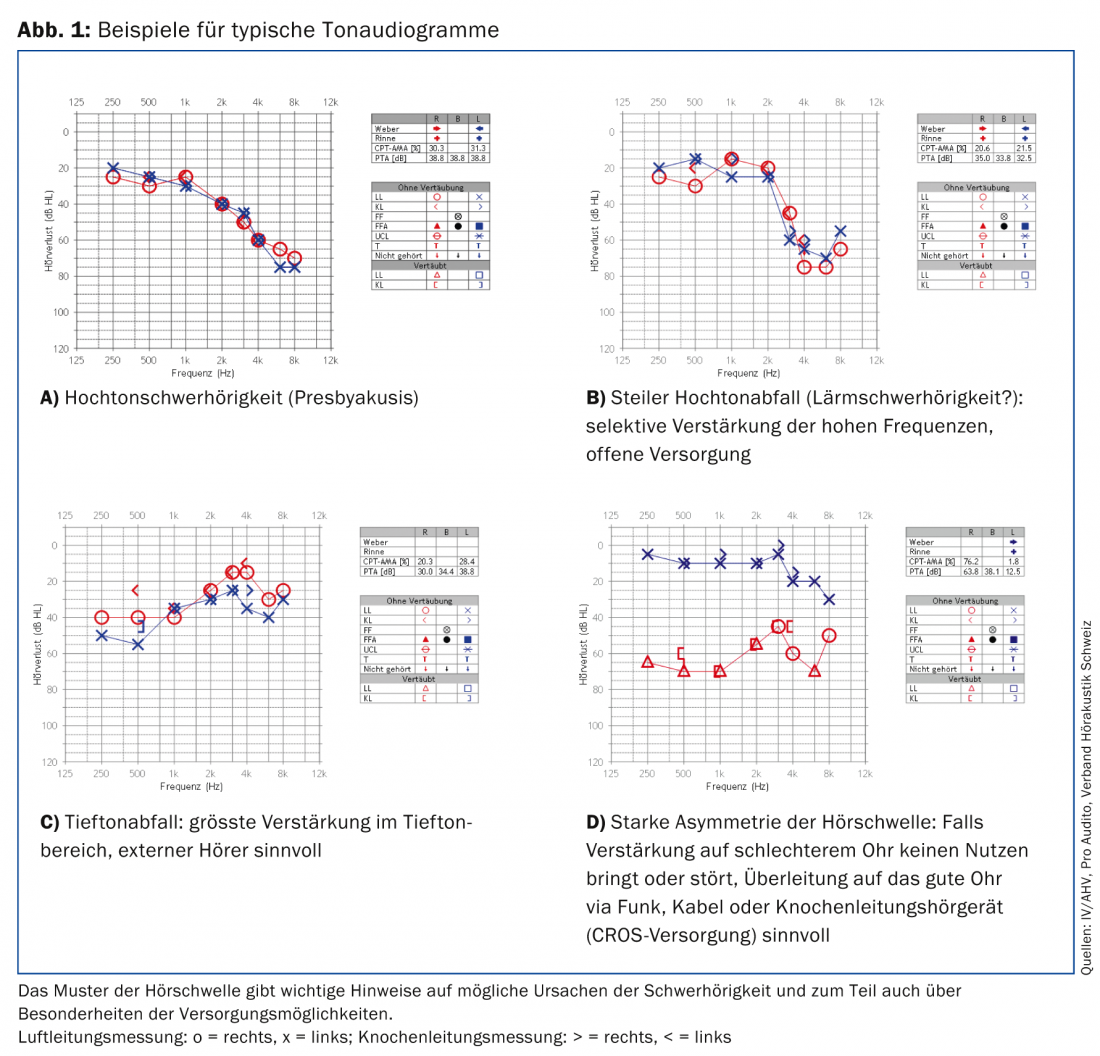
Most hearing losses can be improved with a hearing aid. This is especially true for hearing and speech comprehension at rest. Comprehension problems with background noise are more difficult to correct. Sensorineural hearing loss of all degrees is primarily managed with air conduction hearing aids. For conductive or combined conductive/ sensorineural hearing loss, middle ear surgery with reconstruction of the conductive chain, middle ear implants, or bone conduction hearing aids may be considered. In cases of severe asymmetry of the hearing threshold or unilateral deafness, a transfer to the better ear is performed via radio, cable or through the bone with bone conduction hearing aids. In cases of bilateral profound hearing loss, where the hearing becomes unusable even with hearing aids (hearing loss bordering on deafness), the cochlear implant is the best option.
Figure 1 shows examples of typical hearing losses. The most common hearing disorder is bilateral high-frequency hearing loss in the sense of presbycusis.
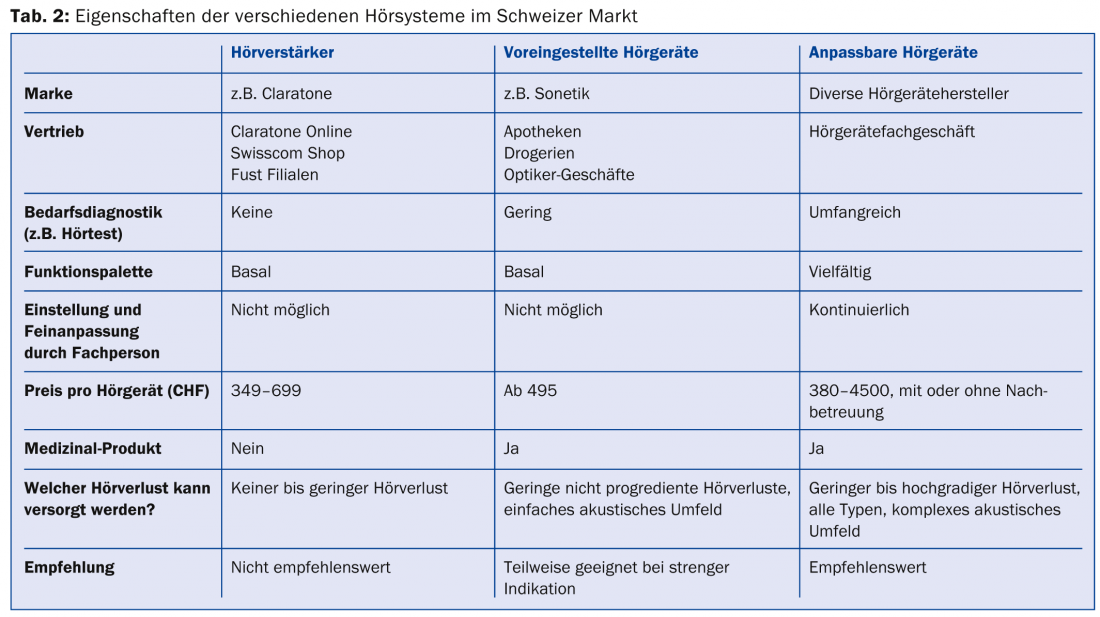
The therapy of choice is air conduction hearing aids. In addition to customizable hearing aids, preset hearing aids and sound processors are also available on the market in Switzerland. Table 2 lists the different product classes.
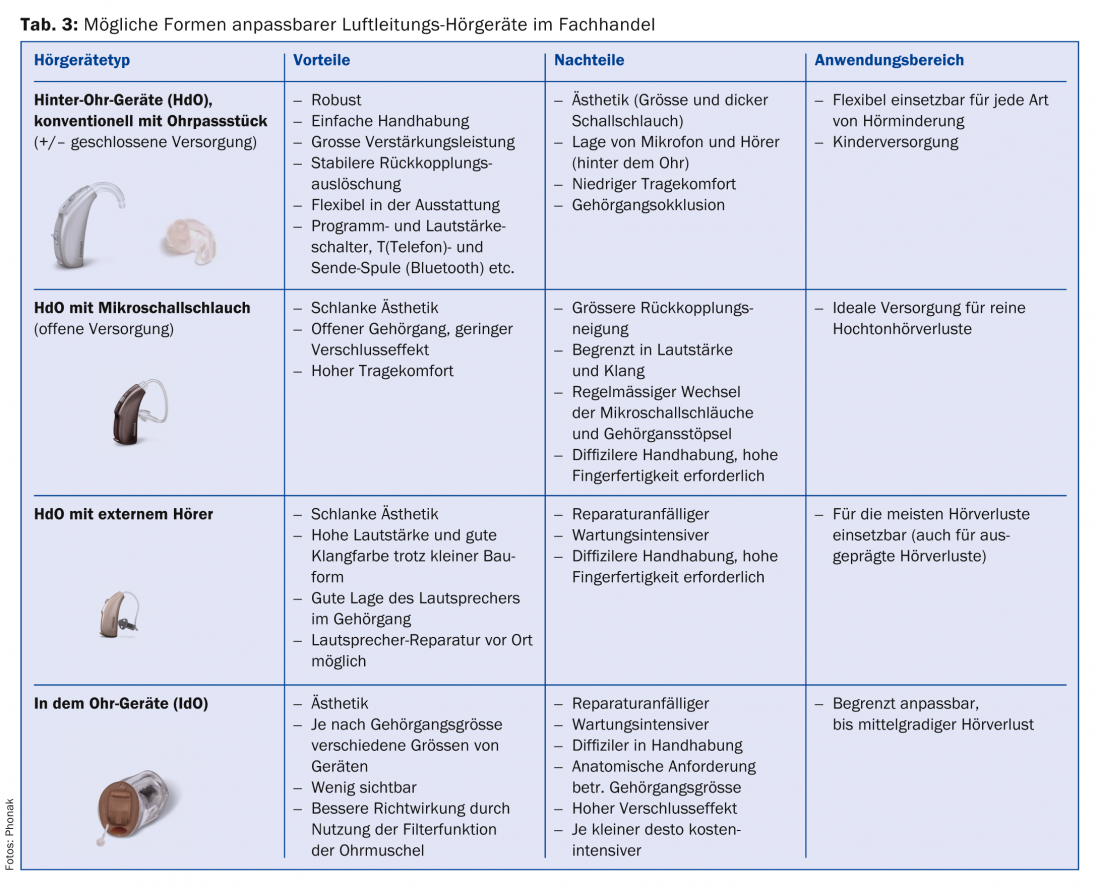
Depending on the hearing loss, acoustic requirements and personal preferences, different designs of hearing aids can be considered (Tab. 3).
Which is the best hearing aid?
The best hearing aid is the one that best fits the hearing loss and the individual’s needs and hearing profile. Fitting a hearing aid takes time, patience and perseverance. The brain, which received less acoustic input over a longer period of time, has to get used to the new situation. It is normal that in the initial phase everything is perceived much too loudly. Today’s hearing aids are hi-tech devices, and a user must invest time to understand and try out the setting options, just as with a smartphone. Testing the setting in daily life and in the individual listening environment is essential, and different hearing aids should be tried.
Mild hearing loss across all frequencies may be able to be accommodated with preset hearing aids or low-cost hearing aids available from specialty stores. However, it is difficult for patients to assess their needs themselves and they are therefore dependent on objective advice from their ear specialist or acoustician. This professional advice is not available in a pharmacy or post office. A non-specialist (e.g., pharmacist) may be able to roughly estimate which type of hearing aid is more likely based on the pure tone audiogram, but further adjustment or subsequent repair is not possible. The IV/AHV/SUVA do not pay a contribution to hearing amplifiers, but they do pay for pre-fitted hearing aids and for regularly fitted hearing aids.
How do simple hearing aids differ from more complex ones?
Sound processors and simple hearing aids offer no or fewer adjustment options than more complex hearing aids. For example, simple hearing aids have only a few channels and thus only allow gain adjustment of a few frequency blocks. More complex hearing aids contain up to 20 channels, which allows selective amplification from frequency to frequency, similar to an equalizer. Other technical features of complex hearing aids include transposition or frequency compression, directional microphones, reverberation and impulse sound suppression, wind noise suppression, and synchronization and data exchange of the hearing aids in the case of binaural fittings.
With the frequency transposition resp. -compression, the incoming sound (e.g. birdsong) is shifted from a frequency range that is inaudible to the person concerned into the audible range. Directional microphones prioritize amplifying sound in one direction and offer a distinct advantage in background noise. The ability to connect the device to accessories such as an external microphone, radio or telephone is also reserved for more complex hearing aids. Wind noise suppression is useful when working outdoors. In cases of pronounced asymmetry of hearing or one-sided deafness, sound must be transmitted from the worse ear to the better ear, for example via radio link.
In the case of complex fittings, it is worthwhile for the patient to apply to the IV as a hardship case in order to be able to obtain better funding for an advanced hearing aid after appropriate assessment at an ENT clinic.
Increasing the quality of life
A successful hearing aid fitting brings not only hearing improvement but also an increase in quality of life. A 2009 Swiss cross-sectional study found that a high proportion (85%) of hearing aid owners use the device regularly; 80% of users are satisfied with the hearing aid [7]. Patients can therefore be motivated without reservation to have their hearing carefully checked and improved accordingly, because with the diverse range of hearing aids and thanks to technical advances, most hearing losses can be satisfactorily treated today. It is important to adapt the hearing aid to the user’s needs, to collaborate with professionals and to have realistic expectations.
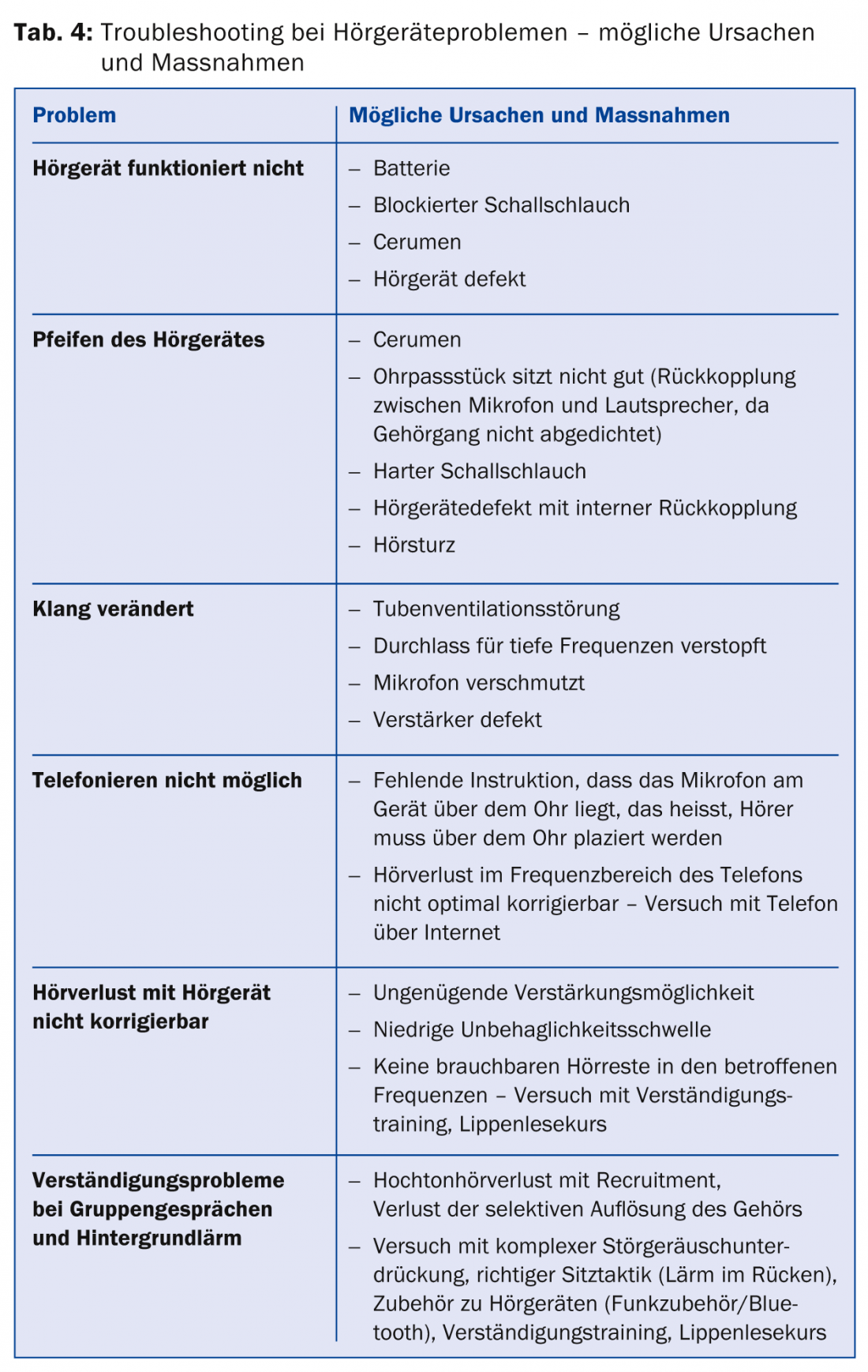
The relationship of trust between the acoustician and the hearing aid user is not only a prerequisite for an optimal fitting, but also for the possibility of comparative fitting of different hearing aids and subsequent continuous readjustment. Many problems can be solved in this way (Tab. 4).
Unfortunately, in 2011, the IV/AHV abolished the final expert opinion after fitting the definitive hearing aid. Nevertheless, in case of uncertainty or dissatisfaction regarding the fitted hearing aids, the patient can seek advice, for example from the ENT physician, from the regional section of pro audito Switzerland or from the ombudsman’s office (also via pro audito).
Conclusion for practice
- Hearing impairment affects those affected; cognitive impairment, isolation, and depression may also follow.
- Impairment is best assessed using speech hearing tests (quiet and noise) and handicap questionnaires.
- The choice of hearing-improving measures depends on the demands on hearing in everyday life and individual needs.
- For the provision of hearing aids, the IV/AHV make a voluntary lump-sum contribution for a total hearing loss per ear >20% (IV) or 35% (AHV).
- From the ENT physician’s point of view, we recommend an optimal fitting of both ears adapted to the needs with maximum possible hearing gain.
- Fitting a hearing aid takes time, patience, and an adjustment effort by the brain.
- Since many hearing disorders are progressive over time, it is generally recommended to purchase an adjustable hearing aid fitted by a professional.
- Pro audito as an association of the hearing impaired supports patients with many questions. Contacting them or becoming a member may well be worthwhile.
Literature
- Chisholm TH, et al: A systematic review of health-related quality of life and hearing aids: final report of the American Academy of Audiology Taskforce On Health Related Quality of Life Benefits of Amplifications in Adults. J Am Acad Audiol 2007; 18(2): 151-183.
- Lin FR, et al: Hearing loss and cognitive decline in older adults. JAMA Intern Med 2013; 173(4): 293-299.
- Arlinger S: Negative consequences of uncorrected hearing loss – a review. Int J Audiol 2003; 42 Suppl 2: S17-20.
- Kramer SE, Kapteyn TS, Houtgast T: Occupational performance: comparing normally hearing and hearing-impaired employeex using the Amsterdam Checklist for Hearing and Work. Int J Audiol 2006; 45(9): 503-512.
- Bertoli S, Probst R, Jordan P: Hearing handicap – an addition to audiometric hearing loss. Results of an exploratory study of auditory communication disorders in the elderly, ENT 1996; 44(7): 376-378.
- Bertoli S, Bodmer D, Probst R: Survey on hearing aid outcome in Switzerland: associations with type of fitting (bilateral/unilateral), level of hearing aid signal processing, and hearing loss. Int J Audiol 2010; 49(5): 333-334.
- Bertoli S, et al: Survey on hearing aid use and satisfaction in Switzerland and their determinants. Int J Audiol 2009; 48(4): 183-195.
HAUSARZT PRAXIS 2015; 10(3): 37-43









