Sports medicine care for active competitive children is an art in itself, and it is important to be well versed in various characteristics of this population. Nowadays, competition-preparatory training is started very early, where children train systematically and several times a week. Just look at the pictures of young artistic gymnasts who are ready for the Olympics while still of school age, which takes eight to ten years of preparation!
Pediatrics for the adolescents, gynecology for the women, geriatrics for the elderly, and sports medicine for the young and older active ladies and gentlemen. That’s about how you might think of the demand in primary care practice, where this diversity of people is coming through the wringer.
But anticipating, it is easier to have a young athlete with his specific problem in front of him and to take care of him than to write about it! Even though there is (almost) no significant gender specificity in adolescents at least until puberty, it makes a difference whether one is dealing with a toddler, a preschool-aged child, a school-aged child, or a prepubescent child – not to mention the not uncommon problems of parents or other adult caregivers (success by proxy). In addition, it must be taken into account that with a calendar age of, for example, twelve years, biological maturity may be observable between 9.5 and 14.5 years. Does this mean that generalization makes sense at all?
In the following, we will briefly highlight two areas: First, specific issues related to training need to be addressed, and then overuse and trauma-related issues need to be discussed.
Strength training for children?
For a very long time, strength training was frowned upon among young people. The rationale was the fear of damaging the delicate growth plates and the more elastic but less pressure and flexion resistant growing musculoskeletal system – but also the argument that with low anabolic hormone levels (especially testosterone) this form of exercise would be ineffective. It is indeed true that until the age of ten/eleven, testosterone levels are low in both sexes and thus the anabolic imprinting remains weak. However, strength training is much more than just promoting muscle fiber hypertrophy; rather, at this age, it is about “neurological” improvement in stimulation of an ever-increasing percentage of muscle fibers, optimized intra- and inter-muscular coordination capacity.
In addition, strength endurance is also improved in this way. Climbing trees or performing a tilt on the parallel bars with an upward swing – both are exercises that require putting your own body weight into motion. But they train not only this feature, but also a sense of balance, coordination and agility. The presumably fragile passive musculoskeletal system benefits from these stimuli, which trigger biopositive adaptation phenomena at the bone. And since the muscles can hardly be overloaded during strength training thanks to control mechanisms, there is hardly any danger from this side either. There are studies that compare the injury rates of training and competition, and strength training comes out far better than track and field or football (0.03 and 0.14, respectively) with 0.012 and weightlifting with 0.013 (cases per 100 hours). However, this general harmlessness is only given if the training is done professionally.
Aerobic and anaerobic training
Specific metabolic capacity is also limited in adolescents compared to adults in the area of anaerobic training (former stamina). Most likely, this is due to the lower activity of glycolytic enzymes in children, especially phosphofructokinase. As a result, lactate elimination and thus recovery capacity is reduced in the child compared to the adult. Nevertheless, this important characteristic may also be trained in a moderate form.
In terms of aerobic endurance exercise, children and adolescents are excellent from a cardiopulmonary and also metabolic perspective . Thus, the thesis at that time of the incompleteness of the child’s heart and the functional limitation of the child’s organism is untenable. However, I would like to point out that due to a steeper slope of heart rate in adolescents and the higher maximum heart rate, some peculiarities must be taken into account when using pulse as an exercise parameter.
Aseptic osteonecrosis
In the orthopedic traumatology field, there are two points that I would like to briefly discuss in this framework.
The first point concerns the aseptic osteonecroses or more modern: the growth osteochondroses, mainly represented by Osgood-Schlatter disease and Sever disease (Fig. 1) .

These conditions are disorders of enchondral ossification with a cause not yet fully known. It is likely that mechanical factors play a major role such as tensile forces due to tendons fixed to apophyses, compressive forces on the growth plate itself, or shear forces on the epiphyseal growth plate. The sport hyperactivity is a favoring factor, but the same applies to the environment where this intense sport is practiced: hard surfaces, artificial grass, rotation blocking sports shoes (studs, nails). Diagnosis of these two most common osteochondroses is clinical (tenderness, distension of the tibial tuberosity in Osgood-Schlatter); radiographs are rarely needed. In Sever’s disease, objectification takes place with magnetic resonance imaging. In both situations, the fixed muscles are usually significantly “shortened” (quadriceps, triceps surae).
Treatment is usually conservative, consisting of indispensable rest, modulation of exercise, stretching of the involved muscles, local physical therapy, and cushioning sole for the sever muscle.
Osgood-Schlatter disease, by far the most common osteochondrosis, is seen in boys about 13 years of age and less frequently in slightly younger girls. Sever’s disease occurs earlier, in children about 9-10 years of age.
Bony tears
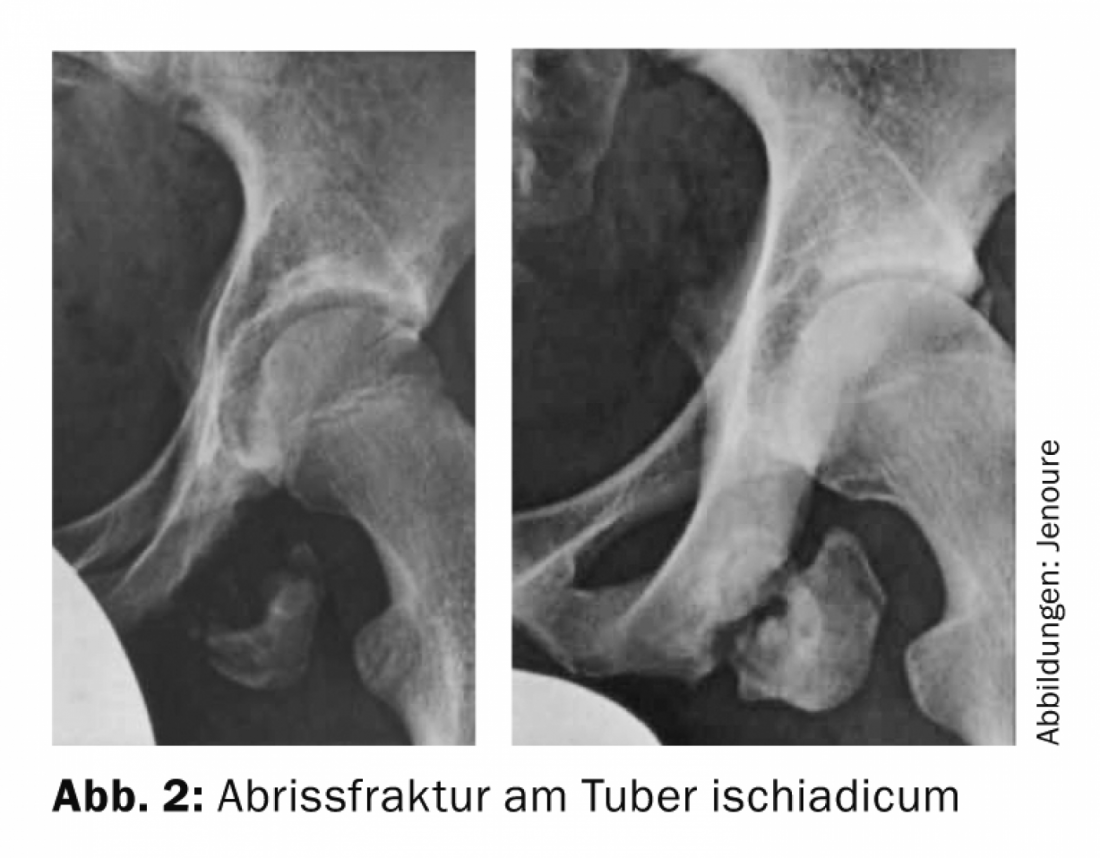
The second point involves bony avulsions, usually at the site of a muscle insertion, which readily leads to confusion with more benign muscle strains. In contrast to osteochondrosis, the onset of which is gradual, these apophyseal avulsions or avulsion fractures are acute events. They are found at the attachment site of the stronger, usually double-jointed muscles, especially of the lower extremity (spina iliaca ant.-superior: M. sartorius/Spina illiaca ant.-inferior: M. rectus femoris/Tuber ischiadicum: hamstrings (flexors)/Trochanter minor: M. iliopsoas/Tuberositas tibiae: patellar tendon → do not confuse with M. Osgood-Schlatter). This injury occurs because the bone is the weaker element of the muscle-tendon-bone functional unit at certain stages.
As can be seen in Figure 2 , the torn bone core also continues to grow. Therefore, it is very important to create a stable reduction at an early stage, surgically if necessary, in such situations that can only be correctly diagnosed with imaging techniques.
In sports, including competitive sports, children develop many important skills and abilities through movement. The stimulated body is the starting point for new experiences. Movement and experience are in turn the basis for the development of intellectual abilities. So favoring sports among young people is almost a duty!
HAUSARZT PRAXIS 2014; 9(8): 6-7