Patients with monoclonal gammopathy of uncertain significance (MGUS) are at increased risk of developing certain forms of cancer. Regular checks allow changes to be detected at an early stage and any necessary treatment measures to be taken in good time. In any case, management must be tailored to the individual risk in order to avoid unnecessary uncertainty.
MGUS is characterized by the detection of increased, complete or incomplete, monoclonal immunoglobulins in a patient’s serum. These are usually determined as “paraprotein” or “M-protein” in serum electrophoresis. However, unlike multiple myeloma, signs of disease such as hypercalcemia, renal insufficiency, anemia, and bone lesions are absent. Although MGUS has no disease value, it may be the precursor of a malignant disease associated with an increase in plasma monoclonal cells, such as multiple myeloma, Waldenström’s disease, or non-Hodgkin’s lymphoma. Often, the main difficulty in management is to correctly identify patients at high risk of progression.
Delimitation and definition
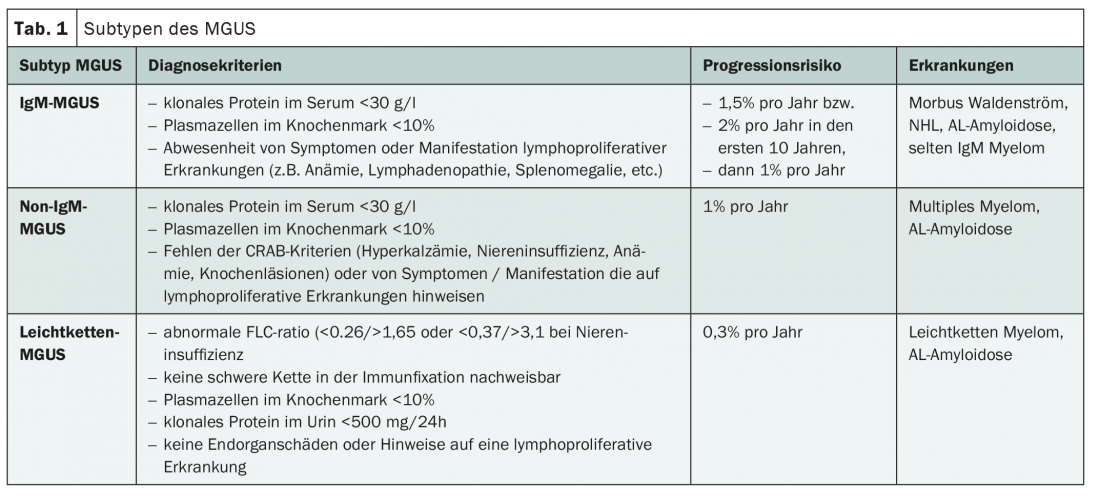
MGUS is defined by a serum IgM protein of less than 30 g/l, less than 10% clonal lymphoplasmacytic cells in the bone marrow, and the absence of symptoms suggestive of multiple myeloma or other B-cell lymphoma. After diagnosis, it must still be clarified whether a plasma cell myeloma is possibly already present. If this is excluded, MGUS is classified into three subtypes (Table 1).
Diagnosis
In addition to a careful history and physical examination, basic diagnostics include a CBC, determination of total protein and albumin in the serum, and quantitative determination of IgG, IgA, and IgM in the blood. If the criteria for MGUS are met, further investigation should follow. In this case, other symptoms suggestive of multiple myeloma requiring treatment must be actively sought and excluded. These include hypercalcemia, anemia, renal insufficiency, and bone lesions – also known by the acronym CRAB. Laboratory determination of electrolytes (sodium, potassium, calcium) and renal values (creatinine including calculated GFR and urea) plays an important role in the analysis of relevant parameters. Since paraproteins can also be deposited as amyloid, and the amyloidosis that subsequently develops mainly affects the heart and kidneys, BNP and NT-proBNP should also be determined.
Risk factors and therapy
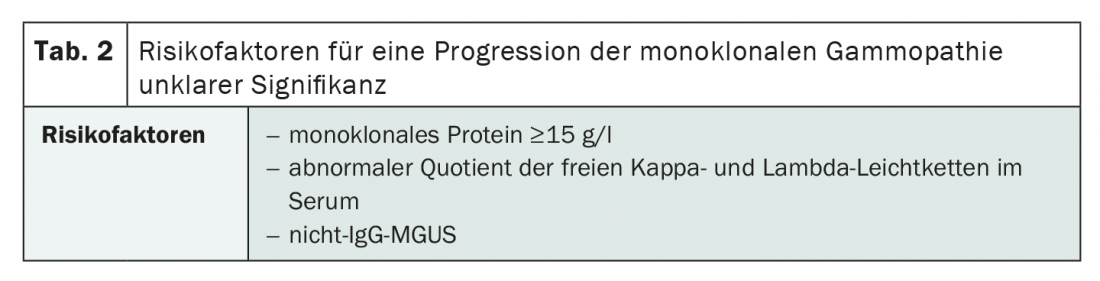
If a more serious disease is suspected, further investigations are required. These are also necessary when high-risk MGUS is present. The most common risk factors for MGUS progression are summarized in Table 2. In the case of low-risk MGUS, however, further examinations are not necessary and are often even counterproductive, as they may cause unnecessary uncertainty in affected individuals.
Unlike multiple myeloma, MGUS is not treated with therapy. Regular check-ups can detect a transition to a disease requiring treatment at an early stage. According to Prof. Jacob Passweg, head of hematology at the University Hospital Basel, this should be done six months after the initial diagnosis. If the laboratory values have not deteriorated in these six months, the interval can be extended to twelve months. In high-risk patients, however, follow-up visits should be performed every six to 24 months. Especially due to the often indolent course, patients at risk should be carefully identified and educated. On the one hand, it is important to avoid secondary diseases. On the other hand, the avoidance of uncertainty is also of great importance.
Source: “Monoclonal Gammopathy of Unclear Significance (MGUS)”, lecture by Prof. Jakob Passweg at the virtual SGAIM Spring Congress 2021, 19.05.2021.
InFo ONCOLOGY & HEMATOLOGY 2021; 9(3): 24-25 (published 6/16-21, ahead of print).