
The benefit of cardiac resynchronization therapy (CRT) varies by QRS characteristics; individual randomized trials are too weak to assess benefit for relatively small subgroups. Accordingly, in a recently published study, a patient-level meta-analysis of randomized CRT trials was performed to assess the relationship between QRS duration and morphology (RBBB, LBBB, or IVCD) and treatment outcomes.
Cardiac resynchronization therapy (CRT) is an important treatment for patients with heart failure, reduced left ventricular (LV) ejection fraction (LVEF), and prolonged QRS duration. Although the results of landmark studies [2–9] have led to widespread use of CRT in many patient cohorts, it is generally recognized that a substantial minority of patients (≈30%) may not benefit from device implantation. Reasons for lack of benefit are varied and include patient factors, electrode placement, and device programming. Although randomized CRT trials originally enrolled patients based on QRS duration (≥120 ms) rather than morphology, many clinicians later concluded that CRT was consistently effective only in patients with QRS duration ≥150 ms [10,11] and left bundle branch block (LBBB) [11–13]. Initially, patients were classified as “non-LBBB,” but further analysis suggests possible differences in patients with intraventricular conduction delay (IVCD) or right bundle branch block (RBBB) [14,15]. Subgroup analyses of individual randomized trials aimed at understanding the relationship between QRS characteristics and CRT benefit were not informative. And observational studies, while informative, are limited by the lack of a control group to help distinguish the effects of treatment from the natural history of disease. Accordingly, in a recently published study, a patient-level meta-analysis of randomized CRT trials was performed to assess the relationship between QRS duration and morphology (RBBB, LBBB, or IVCD) and treatment outcomes [1].
A patient-level meta-analysis was performed of the pivotal CRT trials MIRACLE (Multicenter InSync RandomizedClinical Evaluation) [2], MIRACLE-ICD. (Multicenter InSync ICDRandomized Clinical Evaluation) [9], MIRACLE-ICD II. (MulticenterInSync ICD Randomized Clinical Evaluation II) [3], REVERSE. (Resynchronization Reverses Remodeling in SystolicLeft Ventricular Dysfunction) [6], RAFT (Resynchronization-Defibrillation for Ambulatory Heart Failure ) [8], COMPANION (Comparison of Medical Therapy, Pacing and Defibrillationin Heart Failure) [4], BLOCK-HF (Biventricular Versus RightVentricular Pacing in Heart Failure Patients with AtrioventricularBlock) [5], and MADIT-CRT (Multicenter Automatic DefibrillatorImplantation Trial – Cardiac Resynchronization Therapy) [7].
The primary study outcome was time to hospitalization for heart failure (HF) or death. The secondary outcome was time to death from all causes. All studies included time to HF and death as prespecified end points. While the primary end point varied by study, most studies found a difference in time to HF or death (MADIT-CRT, RAFT, COMPANION, and RAFT). The BLOCK-HF trial was designed to detect a difference in HF, death, or reverse LV remodeling. The MIRACLE studies were based on differences in functional performance and quality of life associated with heart failure.
Characteristics of the overall cohort and subgroups defined by QRS characteristics.
Originally, a total of 7168 patients from eight pivotal CRT trials were included; after application of exclusion criteria, 6261 patients were included in the analysis. The study cohort was older (66 [interquartile range (IQR), 58 to 73] years), predominantly male (75%), had severely reduced LVEF (25% [IQR, 20 to 30]), and had mild or moderate heart failure symptoms (New York Heart Association class II, 52%; New York Heart Association class III, 38%). Common comorbidities included ischemic heart disease (59%), history of hypertension (53%), and diabetes (34%). The most common QRS morphology was LBBB (n=4549 [72,6%]), followed by IVCD (n=1024 [16,3%]) and RBBB (n=691 [11,0%]). Most patients had QRS durations ≥150 ms (n=4122 [66%]). An ICD was implanted in 77% of patients (n=4813), and 61% of patients were randomized to CRT (n=3822). Patients with RBBB were more likely to be male and more likely to have ischemic heart disease. The burden of atrial fibrillation, diabetes, and hypertension and the median ejection fraction were similar in all groups.
Association of CRT with hospitalization or death in heart failure and death overall.
The median [IQR] follow-up time for the overall cohort was 24 months. Randomization to CRT resulted in a reduced risk of HF or death in an unadjusted analysis (HR, 0.73 [95% CrI, 0.65 to 0.82]). Results were similar in an adjusted analysis that accounted for patient characteristics and receipt of an ICD (HR, 0.72 [95% CrI, 0.65 to 0.84]; Figure 1A). Similarly, randomization to CRT resulted in a reduction in all-cause death in unadjusted (HR, 0.77 [95% CrI, 0.66 to 0.92]) and adjusted analyses (HR, 0.78 [95% CrI, 0.67 to 0.94]). There was a significant interaction between randomization to CRT and subgroup QRS characteristics (defined by morphology and duration) as well as HF or death (p<0.001) and all-cause death (p<0.001). Subsequent interaction tests showed a significant interaction between randomization to CRT and a QRS duration of ≥150 ms versus <150 ms for the endpoints of HF or death (p<0.001) and all-cause death (p<0.001), with CRT associated with a significant benefit in patients with a QRS duration of ≥150 ms. In patients with QRS duration ≥150 ms, there was significant interaction between QRS morphology (LBBB, RBBB, IVCD) and HF or death (p<0.001), and borderline significant interaction for death (P=0.054). Unadjusted analyses were performed after stratifying patients into six groups defined by QRS morphology (LBBB, RBBB, or IVCD) and duration (<150 ms or ≥150 ms). In unadjusted analyses, CRT was associated with QRS ≥150 ms in patients with either LBBB (HR, 0.55 [95% CrI, 0.48 to 0.65]) or IVCD (HR, 0.66 [95% CrI, 0.42 to 1.00]). CRT was not associated with lower HF or risk of death in any other subgroup. Overall, the results were similar when assessing the secondary endpoint “death from all causes.”
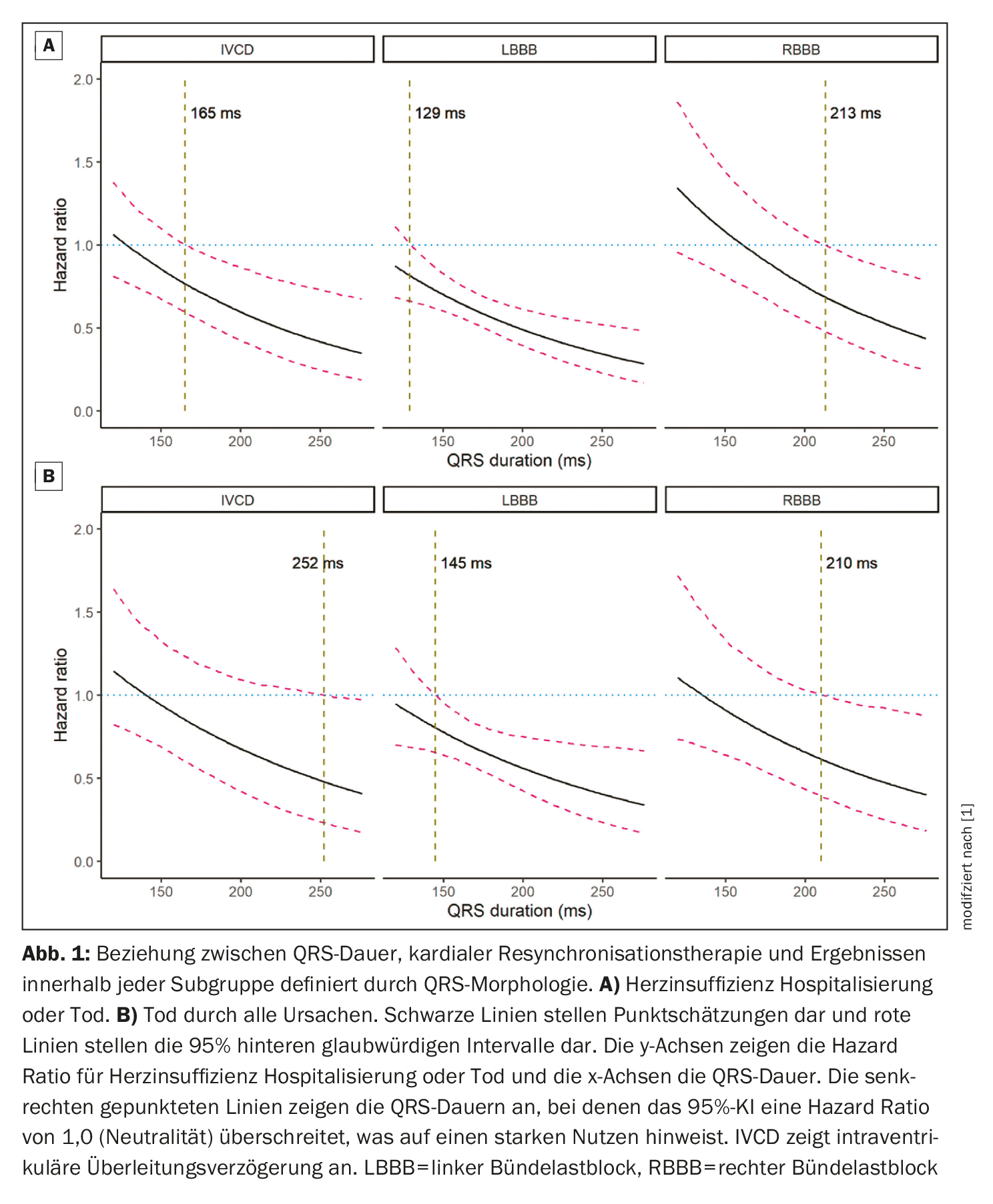
Relationship between QRS duration, cardiac resynchronization therapy, and outcomes.
Adjusted models accounting for patient characteristics and receipt of an ICD were comparable to unadjusted models. CRT was associated with a reduction in HF or death in patients with LBBB and QRS ≥150 ms (HR, 0.56 [95% CrI, 0.48 to 0.66]) and IVCD and ≥150 ms (HR, 0.59 [95% CrI, 0.39 to 0.89]). Whereas there were no statistically significant associations in the other subgroups, the subgroup with LBBB and QRS <150 ms showed a trend toward reduced HF or death, but this was not statistically significant (HR, 0.85 [95% CrI, 0.68 to 1.07]). Results were consistent across studies in adjusted analyses. In addition, the results were similar in adjusted analyses of CRT and all-cause death in the QRS subgroups and across all studies, as well as in sensitivity analyses using frequentist mixed Cox models and in Bayesian Weibull models in which data were removed from the 3 studies with the fewest events. The continuous relationship between QRS duration and CRT benefit was examined for the three QRS morphology subgroups (Fig. 1A) [1]. Among LBBB patients, the 95% CI around HR for the effect of CRT on the composite of HF or death was <1.0 when the QRS duration exceeded 129 ms; in IVCD patients, this duration was 165 ms and in RBBB patients, 213 ms, although the CrI was much greater than in LBBB because of the smaller number of patients and events. Figure 1B [1] shows similar overall results for total death, although the CIs are broader because of the smaller number of events with thresholds of 145 ms, 252 ms, and 210 ms for LBBB, IVCD, and RBBB, respectively. In patients with LBBB, an association between CRT and reduced HF or death was observed when QRS duration exceeded 127 ms in women and 137 ms in men. In patients with IVCD, an association between CRT and reduced HF or death was observed when QRS duration exceeded 140 ms in women and 174 ms in men. In RBBB, CRT may reduce the risk of HF or death if QRS duration exceeds 226 ms in women and 223 ms in men, but the cutoffs were much broader than in LBBB or IVCD.
Take-Home Messages
What’s new?
- In this meta-analysis of patient data, cardiac resynchronization therapy (CRT) was associated with lower rates of hospitalization for heart failure and all-cause mortality in patients with intraventricular conduction delay and QRS duration ≥150 ms.
- The magnitude of CRT benefit in patients with intraventricular conduction delay ≥150 ms and left bundle branch block ≥150 ms appears to be similar.
- There was no clear benefit to CRT in patients with right bundle branch block of any QRS duration, although potential benefit cannot be ruled out in patients with significantly prolonged QRS duration.
What are the clinical implications?
- The practice of combining patients with right bundle-branch block and intraventricular conduction delay into a single “non-left bundle-branch block” category,
to select patients for CRT is not supported by the data. - Patients with an intraventricular conduction delay ≥150 ms should be offered CRT, as is done in patients with left bundle branch block ≥150 ms.
Literature:
- Friedmann DJ, et al: Cardiac Resynchronization Therapy Improves Outcomes in Patients With Intraventricular Conduction Delay But Not Right Bundle Branch Block: A Patient-Level Meta-Analysis of Randomized Controlled Trials. Circulation 2023; doi: 10.1161/CIRCULATIONAHA.122.062124.
- Abraham WT, et al: MIRACLE Study Group. Cardiac resynchronization in chronic heart failure. N Engl J Med. 2002; 346: 1845-1853.
doi: 10.1056/NEJMoa013168 - Abraham WT, et al: MIRACLE ICD II Study Group. Effects of cardiac resynchronization on disease progression in patients with left ventricular systolic dysfunction, an indication for an implantable cardioverter- defibrillator, and mildly symptomatic chronic heart failure. Circulation 2004;110: 2864-2868. doi: 10.1161/01.CIR.0000146336.92331.D1
- Bristow MR, et al: COMPANION Investigators. Cardiac-resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004; 350: 2140-2150. doi: 10.1056/nejmoa032423
- Curtis AB,et al: BLOCK HF Trial Investigators. Biventricular pacing for atrioventricular block and systolic dysfunction. N Engl J Med. 2013; 368: 1585- 1593. doi: 10.1056/NEJMoa1210356
- Linde C, et al: REVERSE Study Group. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J Am Coll Cardiol 2008; 52: 1834-1843. doi: 10.1016/j.jacc.2008.08.027
- Moss AJ, et al: Cardiac-resynchronization therapy for the prevention of heart-failure events. N Engl J Med. 2009;361:1329-1338. doi: 10.1056/NEJMoa0906431
- Tang AS, et al: AFT Trial Investigators. Cardiacresynchronization therapy for mild-to-moderate heart failure. N Engl J Med. 2010;363:2385-2395. doi: 10.1056/nejmoa1009540
- Young JB, et al: MIRACLE ICD Trial Investigators. Combined cardiac resynchronization and implantable cardioversion defibrillation in advanced chronic heart failure: the MIRACLE ICD Trial. JAMA 2003; 289: 2685-2694. doi: 10.1001/jama.289.20.2685
- Bryant AR, et al: Association between QRS duration and outcome with cardiac resynchronization therapy: a systematic review and meta-analysis. J Electrocardiol. 2013; 46: 147-155. doi: 10.1016/j.jelectrocard.2012.12.003
- Gold MR, et al: Effect of QRS duration and morphology on cardiac resynchronization therapy outcomes in mild heart failure: results from the Resynchronization Reverses Remodeling in Systolic Left Ventricular Dysfunction (REVERSE) study. Circulation. 2012;126: 822-829. doi: 10.1161/circulationaha.112.097709
- Dupont M, et al: Differential response to cardiac resynchronization therapy and clinical outcomes according to QRS morphology and QRS duration. J Am Coll Cardiol 2012;60: 592-598. doi: 10.1016/j.jacc.2012.03.059
- Zareba W, et al: MADIT-CRT Investigators. Effectiveness of cardiac resynchronization therapy by QRS morphology in the Multicenter Automatic Defibrillator Implantation Trial-Cardiac Resynchronization Therapy (MADIT-CRT). Circulation. 2011; 123: 1061-1072. doi: 10.1161/circulationaha.110.960898
- Kawata H, et al: Cardiac resynchronization defibrillator therapy for nonspecific intraventricular conduction delay versus right bundle branch block. J Am Coll Cardiol 2019; 73: 3082-3099. doi: 10.1016/j.jacc.2019.04.025
- Sundaram V, et al: Implantable cardioverter-defibrillators with versus without resynchronization therapy in patients with a QRS duration >180 ms. J Am Coll Cardiol 2017; 69: 2026- 2036. doi: 10.1016/j.jacc.2017.02.042.
CARDIOVASC 2023; 22(1): 22-23









