
The 8th Iron Academy was not just about iron per se, but put iron deficiency in a larger practical context. Topics included early detection and management of oncology patients and the renal failure patient in family practice.
According to Prof. Dr. med. Daniel Betticher, Clinic for General Internal Medicine and Clinic for Oncology, Fribourg Hospital, cancer prevention is initially about reducing risk factors through an unhealthy lifestyle (stopping smoking, moderate alcohol consumption, protection from the sun, healthy diet, etc.). The second imperative is early diagnosis. Nonspecific symptoms such as pain, fatigue, asthenia or constipation are much more common than the “red flags”, i.e. specific symptoms such as hemoptysis, melena, alternating constipation/diarrhea, etc. The National Institute for Health and Care Excellence (NICE) dedicated specific guidelines to specific symptoms in 2005. Family physicians in England were instructed to refer patients with these symptoms to cancer centers. It was shown that this could indeed significantly shorten the interval between the first appearance of symptoms and diagnosis in certain types of cancer [1].
But is the shortened interval also associated with better chances of cure (or a longer time between diagnosis and death)? According to a paper by Tørring et al. interval shortening – at least for the specific symptoms – contributes to a lower mortality risk in patients with colorectal cancer [2]. In the area of non-specific symptoms, on the other hand, no significant correlation could be demonstrated. These include fatigue, which is often due to an iron deficiency. One study showed that 42.6% of 1513 cancer patients had transferrin saturation (TSAT) below 20% [3]. 33% were anemic. So when should substitution be used [4]?
- AIDA (“absolute iron deficiency anemia”, e.g. colon carcinoma): TSAT <20%, ferritin <30 ng/ml. Here, i.v. iron is indicated.
- FIDA (“functional iron deficiency anemia, e.g., meat aversion, metastatic gastric carcinoma): TSAT <20%; ferritin 30-800 ng/ml. This group could benefit from i.v. iron supplementation.
- FIDA: TSAT 20-50%, ferritin 30-800 ng/ml. This group is unlikely to benefit from i.v. iron supplementation.
At even higher levels, iron overload is present and iron substitution is not necessary.
Early detection programs
Early detection programs are considered the third cancer prevention imperative. “The goal should be to diagnose the carcinoma before it has fully developed, that is, while it is still moderate or severe dysplasia,” Prof. Betticher said. One example is screening for cervical cancer with diagnosis of precancerous lesions with a simple smear test (every year for the first three years, then every three years). Non-randomized studies showed a decrease in mortality after the introduction of the test. Cervical smear is recommended for all women 21 years of age and older.
Breast carcinoma: Mammography screening looks for early stage carcinoma. In a Cochrane review, randomized trials showed that mortality risk can be reduced by 23% after 13 years. But what is the situation in Switzerland? “If all female residents in Switzerland aged 50-69 years were screened, 160 could be saved from death each year,” Prof. Betticher said. “Compared to ‘wild’ screening, axillary lymph node involvement is 50% less frequent if early detection is organized. This is an often forgotten advantage, because an advanced stage also requires a more intensive therapy. Overall, it can be said that mammography is effective and cost-efficient. Therefore, it is recommended to all women over 50 years of age.”
Colon carcinoma: Examination options for colon carcinoma include detection of blood in stool or (virtual) colonoscopy. The goal is to detect an early stage of development with polyps or early carcinoma that is still curable with surgery and chemotherapy. Blood detection has a proven benefit (it reduces mortality risk by 16% according to a Cochrane review of four randomized trials [5]), but you do miss out on a relatively large amount. The false negative rate is up to 75%. The gold standard is therefore colonoscopy. According to estimates (no randomized trials), this reduces mortality by half and allows resection of polyps in the same session. However, it is a procedure (albeit small) with the corresponding side effects. Virtual colonoscopy does not mean surgery, but it does not allow removal of polyps. In addition, a polyp must be >9 mm in size to be detected with virtual colonoscopy. “Overall, in cases of normal risk or familial predisposition, colonoscopy is advisable from the age of 50 , as the likelihood of carcinoma increases from this point,” Prof. Betticher explained.
Lung carcinoma: In lung carcinoma, it is not possible to identify a precancerous stage. The National Lung Screening Trial (NLST) did show that annual low-dose CT examinations achieved reductions in lung cancer-specific and all-cause mortality (by 20 and 6.7%, respectively). However, there were also a lot of findings that needed clarification. The overdiagnosis rate was relatively high, and the cost-benefit ratio was poor. Therefore, screening is not globally recommended to smokers at this time. It is yet to be determined which is the best screening population.
Prostate carcinoma: Although the Gothenburg study had shown in the field of prostate carcinoma that the mortality risk after 15 years can be reduced by a significant 44% by PSA testing [6]. However, twelve men had to be treated for one to be cured. Morbidity after surgery (urinary incontinence 15-50%, sexual dysfunction 20-70%) or after radiotherapy (urinary incontinence 2-16%, sexual dysfunction 20-45%) is high. Due to the poor specificity and sensitivity of the test, mass screening is not recommended – unless there are clear risk factors (black skin color, father or brother with prostate cancer) or the informed patient explicitly wishes to be screened. The life expectancy must be at least ten years.
The renal insufficiency patient in family practice
According to Prof. Rudolf P. Wüthrich, MD, Clinic for Nephrology, University Hospital Zurich, approximately 500,000 people in Switzerland have an impaired glomerular filtration rate (GFR). The prevalence of chronic renal failure is increasing in the general population. Screening for kidney disease is therefore advisable every one to two years in high-risk groups. These include diabetics, hypertensives, and individuals with a family history of diabetes. Serum creatinine (GFR estimate), protein/creatinine or albumin/creatinine, and urine sediment are measured. At the end of the clarification, the following should be determined:
- Stage and progression tendency of renal insufficiency (serum creatinine, possibly cystatin C, previous values, progression tendency).
- Acute or chronic renal failure? (History; ultrasound: shrunken kidneys, structure, singleness).
- Prerenal, postrenal, renal? (History, blood pressure, jugular veins; ultrasound: obstruction, urine retention).
- If renal: glomerular, tubulointerstitial, vascular? (Sediment, protein/creatinine, urine protein profile, free light chains in serum).
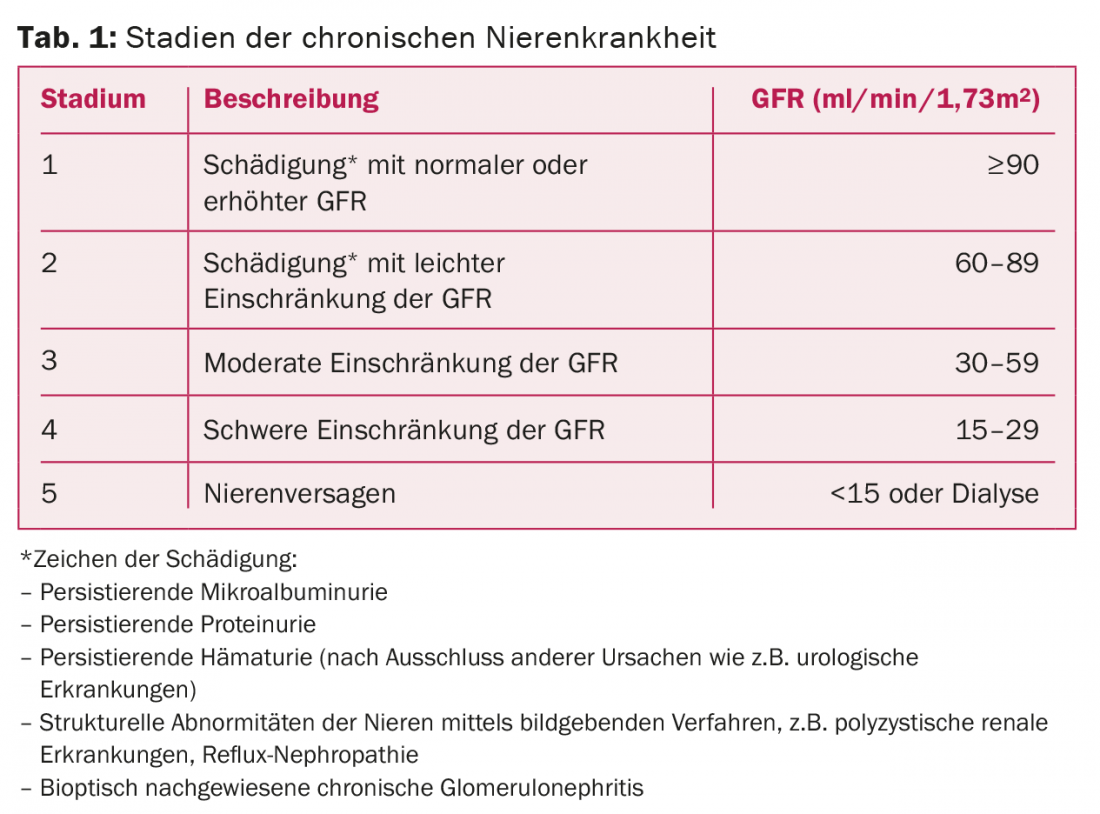
Chronic kidney disease (CKD) is classified into five stages (Tab. 1) . In addition, there is the CGA classification of chronic kidney disease according to underlying disease(causa), glomerularfiltration rate (GFR) and albuminuria. GFR is divided into six categories, albuminuria into three. It has been shown that the risk of mortality in chronic renal failure is dependent on the extent of albuminuria (the higher, the more dangerous).
Avoid progression
Progression of renal failure can generally be inhibited by optimal blood pressure control with ACE inhibitors or angiotensin II receptor blockers [7], statins, and bicarbonate. In this context, double blockade with ACE inhibitors and angiotensin II receptor blockers should be refrained from, as a 2008 study showed [8]. Blood pressure targets in renal disease are values of <140/90 mmHg. In at-risk populations such as patients with diabetes, values of <135/85 mmHg should be targeted, and in chronic nephropathy with proteinuria less than 1 g/d, values of <130/80 mmHg and <125/75 mmHg, respectively (proteinuria >1 g/d). A study by Baigent and colleagues demonstrated a significant reduction in the incidence of severe atherosclerotic events with simvastatin plus ezetimibe in patients with advanced chronic kidney disease [9].
Complications of progressive chronic renal failure are mainly cardiovascular morbidity in CKD stage 2, hyperparathyroidism and anemia in stage 3, metabolic acidosis and hyperkalemia in stage 4, and dialysis in stage 5.
Renal anemia
The pathogenesis of renal anemia is via reduction of nephron mass, resulting in decreased erythropoietin production. Chronic blood loss causes iron deficiency, and malnutrition in turn causes vitamin deficiency. In addition, the erythrocyte half-life is shortened. A hemoglobin level (Hb) <11 g/dL is an indication for therapy (prior to dialysis). Target Hb between 11 and 12 g/dL (or 13), but not higher. Prerequisites are “full” iron stores: ferritin >100 ug/l and transferrin saturation >20%. Iron is administered parenterally (Ferinject® or Venofer®), as this is more rapid and efficient than oral administration [10].
In Switzerland, the erythropoietin preparations Mircera®, Aranesp®, Recormon® and Eprex® are available. When the hemoglobin level rises too high (levels of 13 g/dL and higher), it becomes dangerous as events such as death, myocardial infarction, hospitalization for heart failure, and stroke are clustered [11].
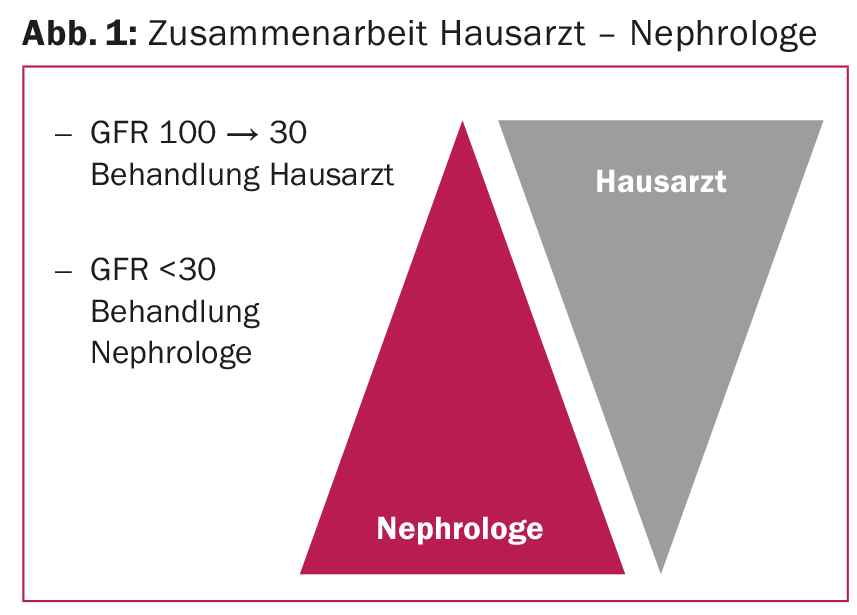
“In general, it is very important that the collaboration between the primary care physician and the nephrologist works well in the treatment of patients with kidney disease,” he said. Figure 1 shows an example of what such an approach might look like.
Source: 8th Iron Academy, April 30, 2015, Zurich-Oerlikon
Literature:
- Neal RD, et al: Comparison of cancer diagnostic intervals before and after implementation of NICE guidelines: analysis of data from the UK General Practice Research Database. Br J Cancer 2014 Feb 4; 110(3): 584-592.
- Tørring ML, et al: Time to diagnosis and mortality in colorectal cancer: a cohort study in primary care. Br J Cancer 2011 Mar 15; 104(6): 934-940.
- Ludwig H, et al: Prevalence of iron deficiency across different tumors and its association with poor performance status, disease status and anemia. Ann Oncol 2013 Jul; 24(7): 1886-1892.
- Gilreath JA, Stenehjem DD, Rodgers GM: Diagnosis and treatment of cancer-related anemia. Am J Hematol 2014; 89(2): 203-212.
- Hewitson P, et al: Cochrane systematic review of colorectal cancer screening using the fecal occult blood test (hemoccult): an update. Am J Gastroenterol 2008 Jun; 103(6): 1541-1549.
- Hugosson J, et al: Mortality results from the Gothenburg randomised population-based prostate-cancer screening trial. Lancet Oncol 2010 Aug; 11(8): 725-732.
- Brenner BM, et al: Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 2001 Sep 20; 345(12): 861-869.
- Mann JF, et al: Renal outcomes with telmisartan, ramipril, or both, in people at high vascular risk (the ONTARGET study): a multicentre, randomised, double-blind, controlled trial. Lancet 2008 Aug 16; 372(9638): 547-553.
- Baigent C, et al: The effects of lowering LDL cholesterol with simvastatin plus ezetimibe in patients with chronic kidney disease (Study of Heart and Renal Protection): a randomised placebo-controlled trial. Lancet 2011 Jun 25; 377(9784): 2181-2192.
- Van Wyck DB, et al: A randomized, controlled trial comparing IV iron sucrose to oral iron in anemic patients with nondialysis-dependent CKD. Kidney Int 2005 Dec; 68(6): 2846-2856.
- Singh AK, et al: Correction of anemia with epoetin alfa in chronic kidney disease. N Engl J Med 2006 Nov 16; 355(20): 2085-2098.
CARDIOVASC 2015; 14(4): 35-37









