
Dry skin conditions are a common phenomenon, especially in the winter months in mid and northern latitudes of the globe due to low humidity. Dry skin (xerosis cutis) is also a common symptom in various chronic skin diseases, especially in atopic eczema or psoriasis. In these diseases, environmental factors such as dry winter weather or too frequent hand washing, bathing/showering can further worsen skin dryness.
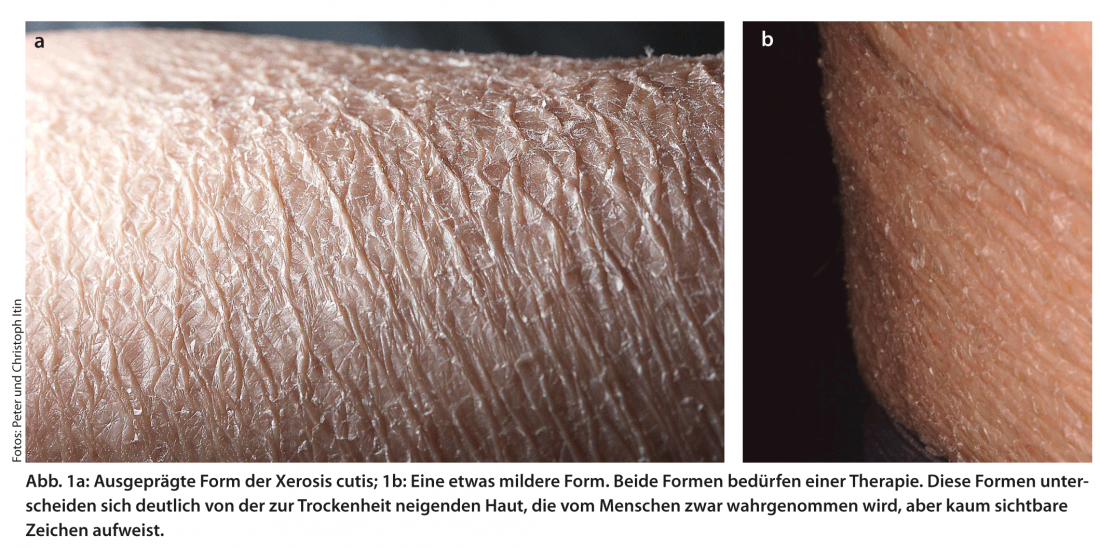
Although xerosis cutis is not threatening, it often places a not inconsiderable burden on those affected; dry skin scales, can look unsightly, not infrequently leads to itching and has an overall negative impact on quality of life (Fig. 1).
Although almost all people know the symptom of dry skin from their own experience, the majority of middle-aged to elderly people are affected – the prevalence is between 40 and 80%. Against the background of the significant increase in the proportion of older people in our society(www.un.org/esa/population/publications/publications.htm), the symptom of dry skin will continue to gain in topicality.
What is dry skin?
The cause of dry skin is a disorder of epidermal differentiation, which leads to a reduced content of intercellular lipids and natural moisturizing factors in the horny layer (stratum corneum). A healthy horny layer contains 15-20% water. If the water content falls below 10%, it becomes flaky and feels dry and brittle. The decreased water content is accompanied by increased transepidermal water loss (TEWL). The mechanical elasticity of the horny layer decreases rapidly (elastic → brittle) and is immediately perceived by the affected person through the changed feeling of the skin. The brittle horny layer becomes flaky, and microcracks form in addition. The latter form entry ports for potentially harmful substances and microorganisms. The disorder is often accompanied by itching.
In addition to intrinsic and genetic factors, environmental factors are often responsible for the occurrence of dry skin. These include above all the reduced humidity in the winter months, but also “lifestyle” or work-related behavior such as frequent hand washing, showering/bathing, staying in air-conditioned rooms, wet work or excessive mechanical stress on the skin, e.g. through clothing.
Dry skin treatment
Measures leading to normalization of epidermal differentiation are the first priority. Changing “lifestyle” or work-related behavior can significantly improve the symptom of dry skin after just a few days and weeks.
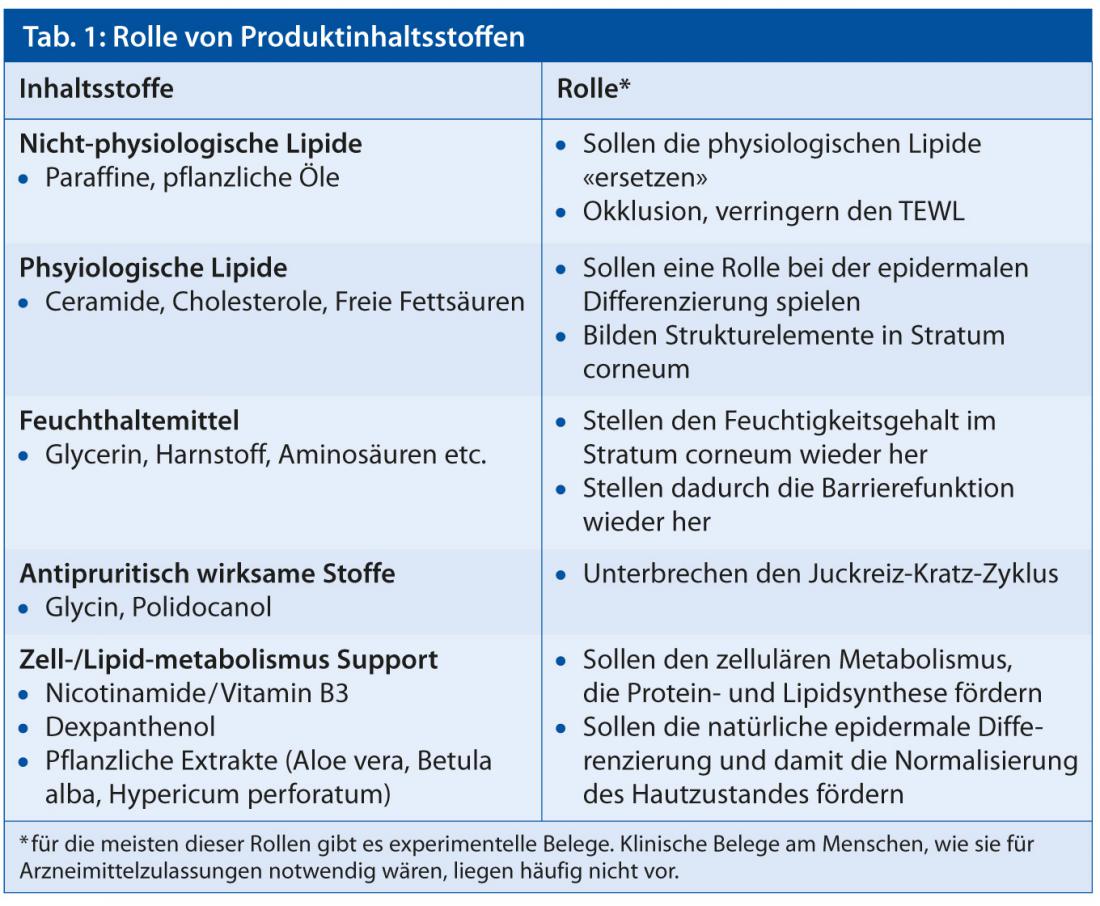
An extrinsically initiated normalization of epidermal differentiation – referred to in the literature as the “inside-out approach” – is attempted to positively influence epidermal differentiation by means of topically applied substances (dexpanthenol, physiological lipids, e.g. ceramides) (Tab. 1). However, no double-blind placebo-controlled studies in humans are currently available.
The products most commonly used today develop their effect through their occlusivity, the topical supply of humectants and the lubrication of the skin surface – referred to in the literature as the “outside-in approach”. Through occlusive lipids – kerosenes, silicone oils, vegetable oils – as well as hygroscopic molecules (humectants) such as glycerin, urea etc., the water content of the horny layer is increased. This temporarily closes microcracks. The degree of occlusivity and moisturization of the horny layer depends primarily on the type and concentration of lipids and humectants used. The effect on humans, based on at least partial restoration of the mechanical elasticity of the horny layer and reduction of transepidermal water loss, is well documented in the literature. Depending on the formulation, there are partly considerable differences.
Today, additional substances are increasingly added to the products to further enhance their effect. Antipruritic substances such as glycine and polidocanol or ingredients such as nicotinamide/vitamin B3 and plant extracts (Aloe vera, Betula alba, Hypericum perforatum) designed to stimulate epidermal differentiation, the production of intercellular lipids and natural moisturizing factors are used. However, appropriate double-blind, placebo-controlled studies in humans are often lacking here as well.
Dry skin as a disease
Although everyone is familiar with the term dry skin, the phenomenon is difficult to narrow down. Drawing the line between pathologically dry skin and skin prone to dryness is experimentally and semantically difficult.
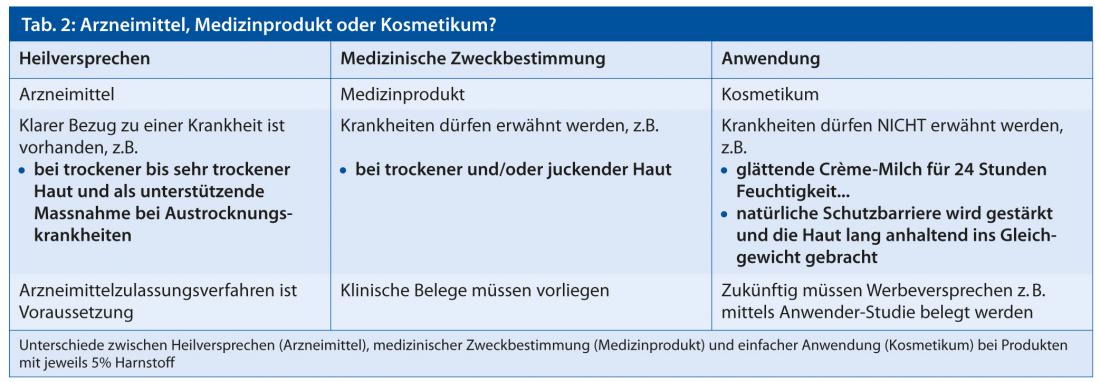
Today, the data situation is often insufficient to market corresponding products as medicinal products with the promise of a cure for the treatment of pathologically dry skin. The cost of large-scale drug trials is enormous. Against this background, companies sell the majority of products in the regulatory status of cosmetics. The evidence for a clinical effect is often scientifically insufficient or non-existent. For the consumer, it is often difficult to interpret the meaning of therapeutic promise (drug), medical purpose (medical device) and ease of use (cosmetic) ( Table 2).
Something else about the terminology of products for the treatment dry skin
Many articles (brochures, flyers, commercials, etc.) make recommendations on properties of products for the treatment of dry skin. The terminology of products for the treatment of dry skin is not infrequently applied inconsistently depending on the target group (consumer, professional) and country/region.
The galenic form itself (ointment, cream, etc.) has little significance for the effect of a product, but only the sum of the ingredients that remain on the skin after application. Lipid-rich ointments and creams are therefore more suitable than lipid-poor ointments and creams. Due to their matrix (emulsion), creams are generally easier to spread and are perceived as more pleasant by the user. It would make sense to label the products with their lipid content.
Products for the treatment of dry skin are often called emollients. In the English-speaking world, the majority of the word emollient is understood as a property of an ingredient. Emollience stands for “softening and softening” and aims to improve the mechanical properties of the horny layer. The term demulcent is hardly used. Demulcent stands for (stimulus) alleviating and aims to reduce stimuli in the microcracks. Humectants are hygroscopic molecules that increase the moisture content of the horny layer and thus improve its mechanical properties. The term moisturizer, used in English as well as in German, colloquially refers to products that moisturize the skin. However, it remains hidden to the user how the product works – through occlusivity or through humectants.
The sensory system is crucial for a successful therapy
Adherence to therapy in patients with pathologically dry skin is comparatively poor. The sensory properties of the topically applied products play an important role. Properties such as absorption behavior, spreadability and skin feel after application are very important for the patient, although they are not primarily relevant for efficacy. Formulations of the O/W type usually perform better in this respect than bases with a lipophilic outer phase (W/O type). Easy and pleasant application can be achieved by sprayable emulsions or foam preparations. Another important factor in the subjective evaluation of products is their odor. From experience in the cosmetics industry, we know that consumers usually prefer a pleasantly scented product to an unscented one. However, fragrances can have an allergenic effect: In favor of better tolerance, the additive should therefore be avoided for sensitive persons.
Prof. Dr. phil. nat. Christian Surber









