Typical symptoms of Ledderhose disease are irritation and pain in the area of the inner edge of the foot. It is a rarely occurring disease of the connective tissue at the plantar fascia. In the area of the tendon there is a more or less nodular or flat hardening. The corresponding changes are clearly visible on magnetic resonance imaging.
In 1894, the German surgeon Georg Ledderhose was the first to report on a usually painful connective tissue deposit of the plantar aponeurosis. Like Dupuytren’s disease of the hand, benign Ledderhose’s disease is classified as a fibromatosis, a benign soft tissue neoplasm. Typically, the disease progresses in episodes over several years [4,5]. Nodular or strand-like connective tissue formations develop in the plantar aponeurosis, which are painful and affect the ability to walk. On clinical examination, these changes are usually palpable and a pain response can be provoked. The exact cause of plantar fibromatosis, also classified as extra-abdominal desmoids, is not known [2,7]. Several medications, such as phenobarbital or primidone, can trigger Ledderhose M. as a side effect.
In addition to conservative symptomatic medication and physical therapy, orthovolt therapy is also promising in the early phase of the disease [3]. Pain reductions can be achieved in about 70% of cases with a subjectively satisfactory course. The therapy is repeatable and well tolerated. Reliable studies of single experimental fibrinolytic injections in plantar fibromatosis are not yet available.
If conservative treatment is frustrated, surgical therapy is indicated. Partial or total plantar fasciectomy can be performed [1]. However, partial ectomy shows a high recurrence rate and more complications than radical surgery.
Radiographs have no value in detecting Led-derhose M. . They can help in the differential diagnosis of plantar pain (plantar calcaneal spur, march fracture, descent of the arch of the foot).
Computed tomographic examinations are also of secondary importance in the visualization of fibromatosis of the plantar aponeurosis because of the lower soft tissue contrast compared with MRI. The differential diagnostic value corresponds to that of X-ray examination, with better detection of fractures.
Magnetic resonance imaging shows fibromatosis with typical signal change [6] of nodular structures, primarily in sagittal and axial sequences. Intravenous administration of Gd-DTPA provides good visualization of the activity and extent of the inflammatory component. In principle, plantar soft tissue disease is best detected by MRI of all imaging modalities.
Case study
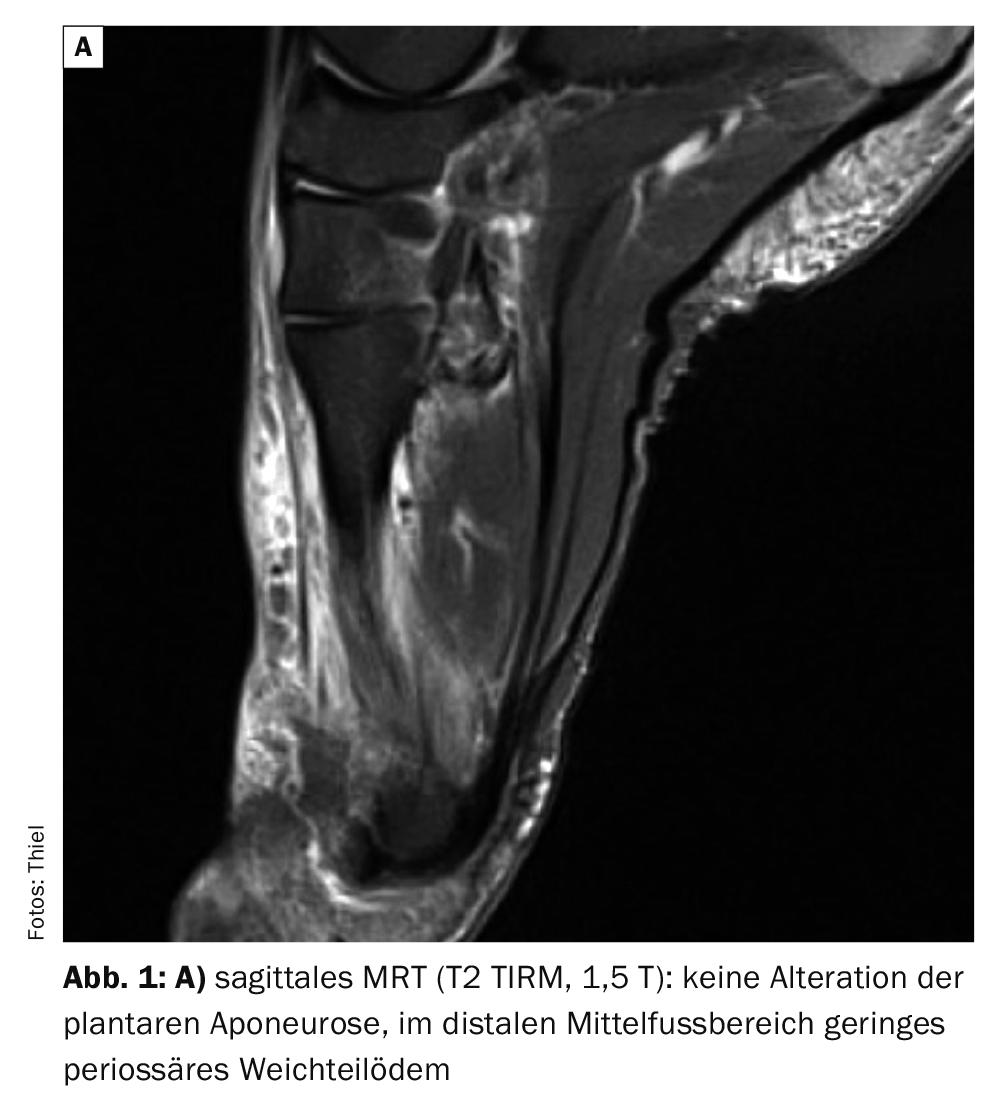
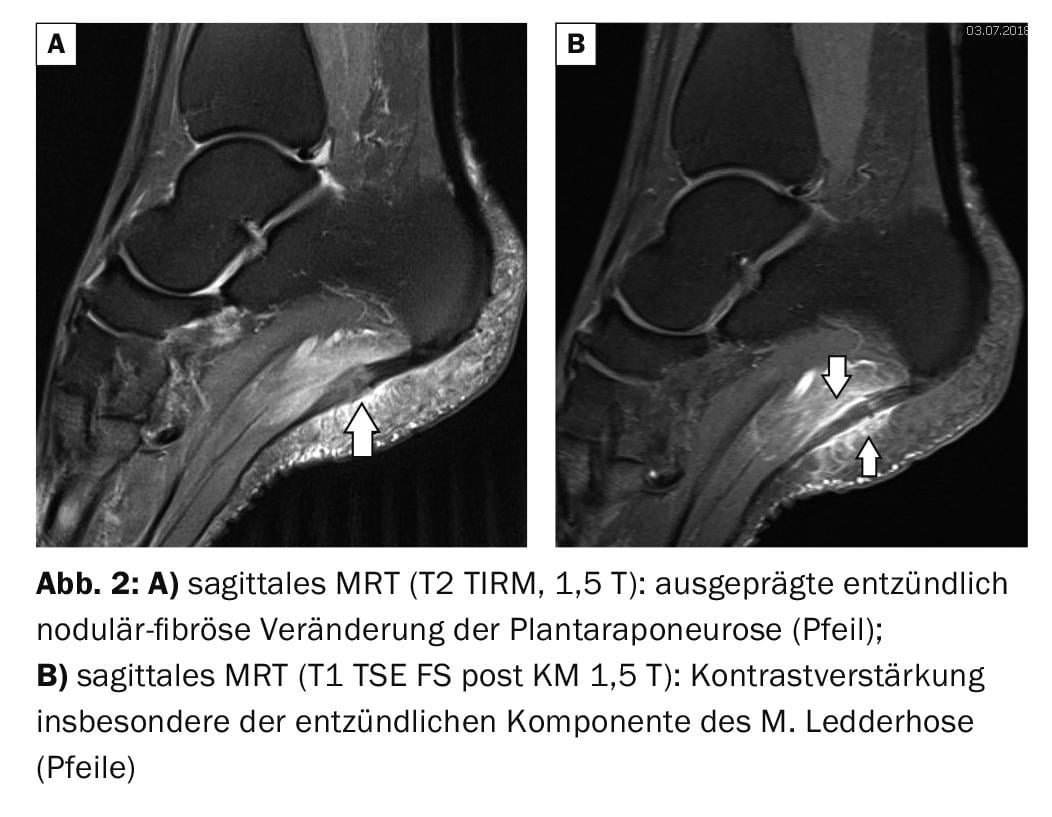
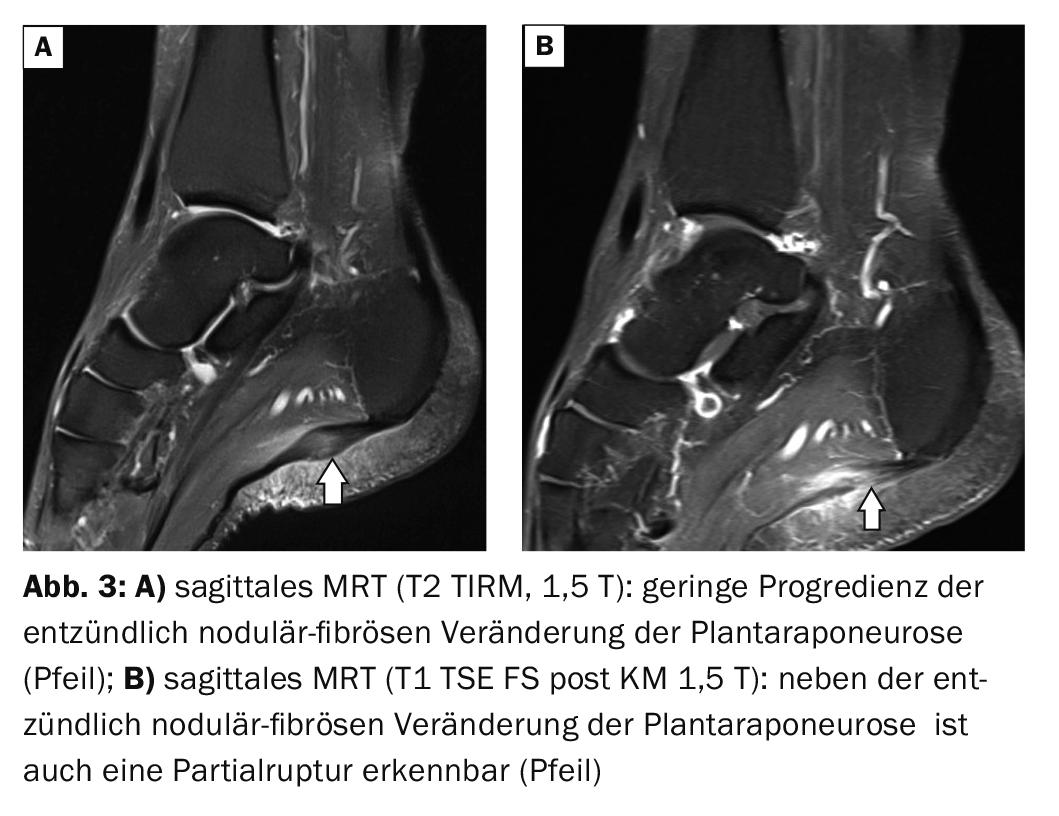
The case report shows the course of Ledderhose disease in a now 56-year-old female patient who first complained of load-dependent plantar pain at the age of 45. The mechanical stress on the foot was high as a medical assistant and full-time employee in surgical practice. The initial MRI of the foot showed no relevant changes (Fig. 1A). With persistent symp-to-matic, an X-ray examination (Fig. 1B) of the right foot was performed about 6 months later with unremarkable findings. In 2018, another MRI (Fig. 2A and B) for chronic recurrent plantar pain demonstrated findings of Ledderhose disease. With insoles and drug analgesic and antiphlogistic treatment, a relatively acceptable situation was achieved until an exacerbation of acute symptoms reappeared in early 2021. The control MRI demonstrated a slight progression of fibromatosis of the plantar aponeurosis and a locally pronounced inflammation (Fig. 3A and B) . The orthovolt therapy already offered in 2018 as a result of the MRI examination, which the patient did not want at that time, was now gratefully accepted by her.

Take-Home Messages
- Ledderhose disease is a benign fibromatosis of the plantar aponeurosis.
- Typical are load-dependent pains in the area of the sole of the foot. The nodular changes can often be palpated and tenderness may be elicited.
- Imaging technique in the detection of plantar fibromatosis is magnetic resonance imaging, the contrast-enhanced sequences can visualize the inflammatory activity very well.
- In addition to conservative treatments, local orthovolt therapy has a very good chance of improving symptoms in the early phase of the disease. Operatively, complete plantar fasciectomy has become widely accepted.
Literature:
- Beckmann J, et al: Plantar fibromatosis: therapy by total plantarfasciectomy. Zentralbl Chir 2004; 129(1): 53-57.
- Carroll P, et al: Plantar fibromatosis: Pathophysiology, Surgical and Nonsurgica Therapies: An Evidence-Based Review. Foot Ankle Spec 2018; 11(2): 168-176.
- Heyd R, et al: Radiation therapy for early stages of morbus Ledderhose. Strahlenther Onkol 2010; 186(1): 24-29.
- Wikipedia: https://de.wikipedia.org/wiki/Morbus_Ledderhose, (last accessed 07.10.2021)
- Parnitzke B, Decker O, Neumann U: “”Ledderhose” disease. Plantar fibromatosis — clinical aspects. Zentralbl Chir 1991; 116(8): 531-534.
- Stoller DW: Magnetic Resonance Imaging in Orthopaedics & Sports Medicine. Second Edition. Lippincott – Raven Publishers. Philadelphia, New York: 1997; pp. 1312.
- Veith NT, Tschernig T, Histing T, Madry H: Plantar fibromatosis – topical review. Foot Ankle Int 2013; 34(12): 1742-1746.
HAUSARZT PRAXIS 2021; 16(10): 42-43