
A discreet lifting effect of the face and stable contours with naturalness of the lips are more in demand today than ever. Rheologically optimized hyaluronic acid (HA) gel products are now available for every region. Various injection techniques are didactically developed to be easy to learn. However, further evidence-based long-term studies extending beyond 12 months are required to better assess empirical values of positive and negative effects of HA gel durability and its rheological behavior. Rare adverse events should be carefully reviewed, documented, reported, and shared with experienced colleagues in expert forums. HA filler and off-label users of botulinum toxin A products in and around the lip region should be aware of the side effects, regularly attend injection training, and recapitulate anatomical knowledge in cadaver courses. Always being “up to date” is the safest way for practitioners and patients.
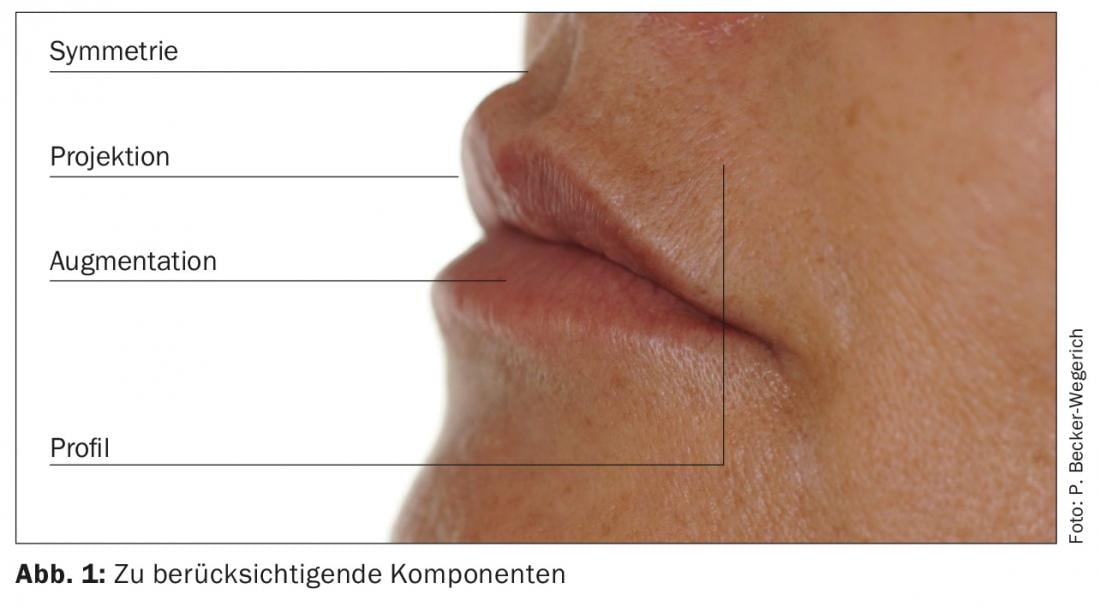
In the theoretical first part of the training series, which appeared in the last issue of DERMATOLOGIE PRAXIS, it was shown what changes the lips and lip environment are subject to in the aging process. Now we are talking about the practice of filler treatment in this area of the face. Components that must be considered when injecting the lips are: Profile, Projection, Augmentation and Symmetry (Fig. 1) .
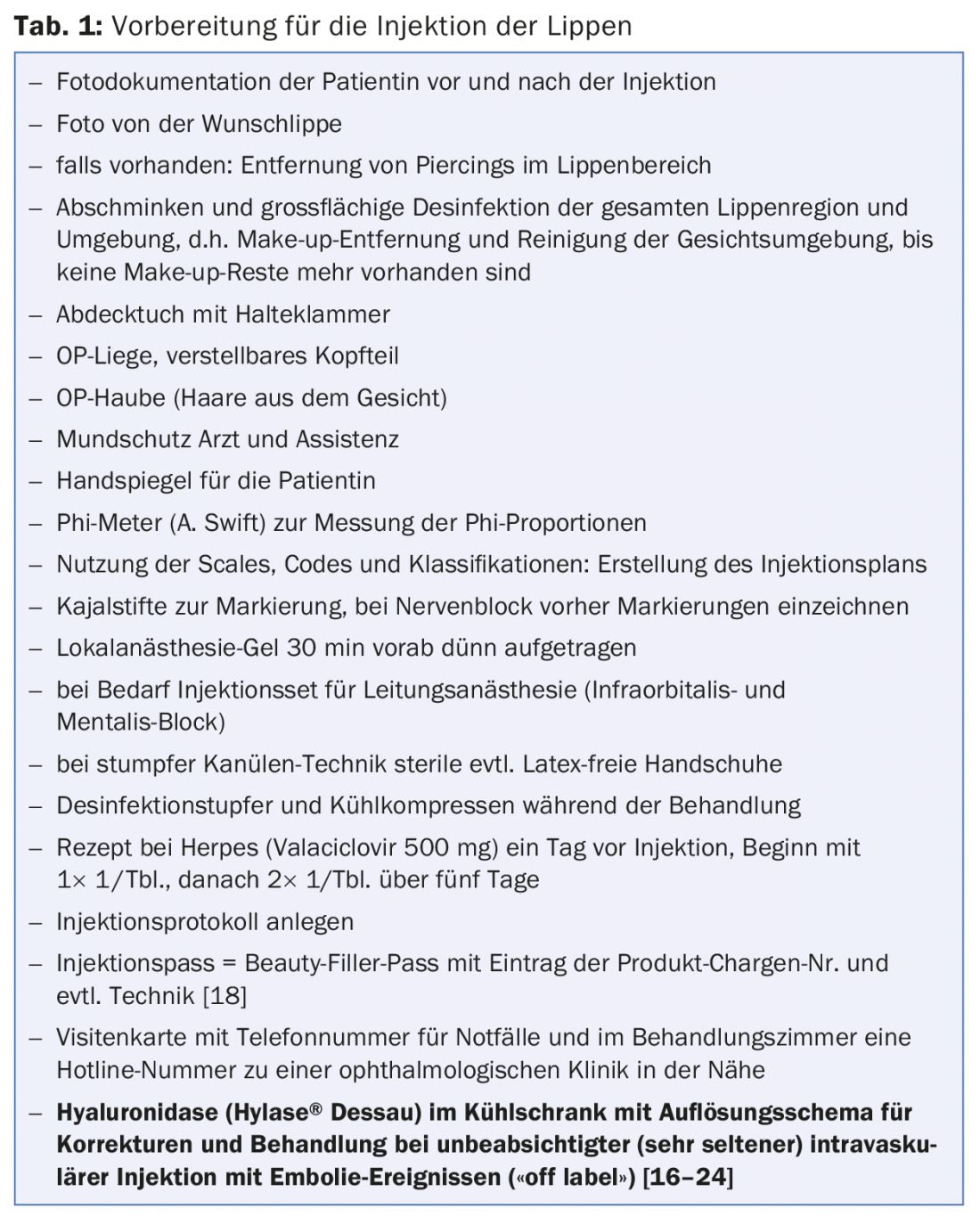
The practical procedure before HA treatment is shown in Table 1.
Variety of lip injection techniques
Of more than 18 injection techniques, the most interesting and helpful can be found in publications or studies [1–17]. It should be taken into account that most practitioners freely combine self-developed creations with these techniques.
MD-Codes™ – highlight for beginners and advanced users
A highlight is Mauricio de Maio’s book [7], reissued at the end of 2015. He has succeeded in developing MD-Codes™ for the face and its anatomical units. Developed at the highest level, this tool is simple and effective for users to learn individualized safe planning and treatment. The MD-Codes™ are tailor-made with their special terminology to the units and structures of the face and are specifically intended for the Juvederm®-Vycross® Collection and its versatile usability. The anatomical units are represented in letters, the subunits of the anatomical units are represented with numbers, and the side of the face is represented by r (right) and l (left). The numbers are superscript and subscript (e.g. Lp1=upper lip red; Lp1=lower lip red). Injection points are also shown in color. In a specific unit, the sequence is numbered. Structures with required high attention or danger (e.g. nerves) are marked in red, like in car traffic the stop signs and prohibition signs.
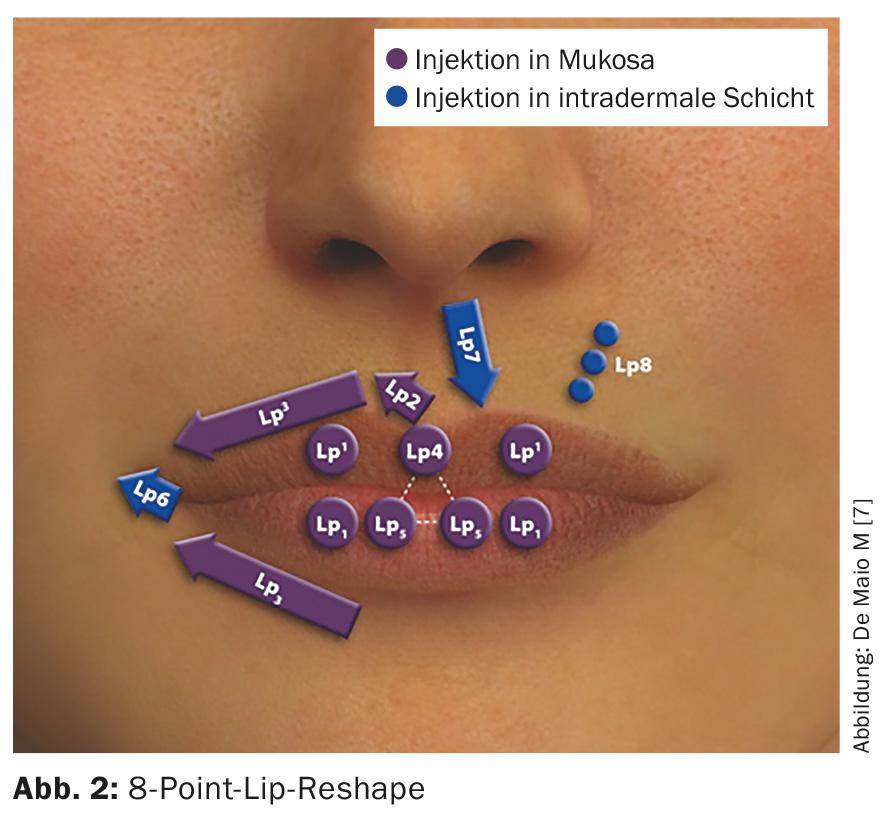
The 8-point lip reshape code (Fig. 2): The MD-Codes™ of the lower facial region are shown in synopsis. For the lips, a diagram with an 8-point lip shaping shows the way to easy handling. The 8-point lip code includes the two letters Lp for lip, superscript numbers for the upper lip and subscript numbers for the lower lip. The injection level into the mucosa is shown in purple, and into the intradermal layers in blue. The start should always be at LP1, then the sequence of numbers up to LP8 can be handled step by step. Three tables are given for lip shaping. Each table clearly shows the products and injection levels matching the code Lp1-Lp8 (marked in blue and purple). Likewise, the volume amount in ml, the injection technique, and the needle or cannula recommendation are shown.
Basic injection techniques
Some basic injection techniques are shown in Figure 3, and include:
- linear technique (retrograde injection) with sharp needle or blunt cannula
- Point technique (retrograde injection) with sharp needle
- Fan technique with blunt cannula or sharp needle (retrograde injection)
- Tunnel technology
- vertical technique (retrograde injection) with sharp needle
- No-touch technique: two to four injection ports without mucosal contact

Products and injection levels for the lip and perioral area are: Emervel® Lips (submucosa, intramuscular, postmuscular), Emervel® Classic (middle dermis), Emervel® Deep (deep dermis), Restylane® (middle dermis), Restylane® Perlane (deep dermis, supraperiosteal), Volbella® (submucosa, intramuscular, postmuscular), Volift® (deep dermis), Voluma® (supraperiosteal), Belotero Balance® (submucosa), Belotero Intense® (deep dermis, subcutaneous) and Belotero Volume® (supraperiosteal, subcutaneous). HA products may contain anesthetics (0.3% lidocaine).
The injections with the pointed needle can lead to an unintended intravascular injection, even in the case of unpredictable anatomical variants of the vessels. The recommendations for higher injection safety are aimed at the use of flexible or rigid cannulas with a blunt tip and lateral opening (e.g., from 25-22 gauge). They are more tissue-friendly, atraumatic and glide more painlessly in the corresponding tissue layer. With only a few stitches, the even distribution of hyaluronic acids is possible.
Procedure in practice
Careful shaping and definition of the lip rim (Fig. 4 and 5):
- light volumizing of the margin: following the given margin along the upper lip subcutaneously above the margin or directly in the lip margin or directly below the lip margin in the lip red (for even proportioning also treatment of the margin of the lower lip)
- gradual treatment for narrow lips or young women: first volume definition for projection and eversion of the red of the lips and then (fine correction after two to four weeks) the edge, if necessary
- Start at the lower lip to respect the anatomical aesthetic relationship of the upper lip to the lower lip.
- With cannula: 5 mm lateral to the corners of the mouth; 25-22 G cannula; retrograde injections along the lip margin (along the entire route omitting the cupid’s bow); HA flows as if in a canal during retrograde injection.
- With the needle: along the lip redline at the level of the rim at 1-cm intervals, one retrograde injection each; two entry points per side at an angle of 30°; vertical injections one entry point next to the others in the lip redline, one drop each HA 2 mm below the lip redline subcutaneously; upper lip and lower lip, if necessary.

Upper lip wrinkles
- With needle (30 G): Entry point white upper lip; vertical injection intradermally; blanching injection technique with Belotero® Soft or, for deep wrinkles extending into the red of the lip, Belotero® Balance.
- With the cannula: entry point white upper lip; 5-10 mm above the lip margin next to the corner of the mouth; for very deep radial folds, fan technique (or linear subcutaneous 25 G or 30 G).
Mouth corner augmentation
- With cannula or needle: entry point 5 mm next to corner of mouth; with 25 G fan technique along a triangle with the cannula or needle (little HA).
Philtrum projection
- With the needle: entry point at the highest point of the cupid’s bow on both sides; along the V-shaped indicated columens; vertical, retrograde linear, intradermal injection technique.
Lip red (vermillion) moistening without projection while maintaining natural convexity.
- With the cannula: entry point 5 mm lateral corner of the mouth or in the red of the lips; area-wide injection directly under the mucosa; fan technique 25 G
Mona Lisa Smile and Cupid Bow Peak Point
- With the needle (30 G): Entry point corner of mouth or arrow-shaped around corner of mouth or one volume point 0.025 ml per side vertically dermal (e.g. Emervel® Lips or Classic or Belotero® Balance, Volbella®); cupid’s bow tips on both sides one volume point 0.025 ml.
Lip volume
- With the needle (30 G): Entry point 2-5 mm above the lip margin of the upper lip and, if necessary, in the case of the lower lip, two to four entry points deep behind or in the orbicularis oris muscle (MOO) at the level of the mucosal tooth termination row (one HA bolus each of 0.1-0.15 ml); needle bevel downward; retrograde HA delivery while injecting slowly from the inside to the outside, delivering less and less, while slowly guiding the needle to the border of the lip redline, then finish injection (=projection points two to four); vary the amount according to the projection wish; light massage
- With the cannula (25 G): Entry point 2 mm next to the corner of the mouth; linear retrograde injection technique deep behind the MOO (eversion).
Possible side effects and precautions
The development of new three-dimensional volume building and contouring techniques, as well as deeper and more extensive injections, requires precise knowledge of the anatomy. Thus, side effects are very rare and mostly temporary. Product safety levels are high.
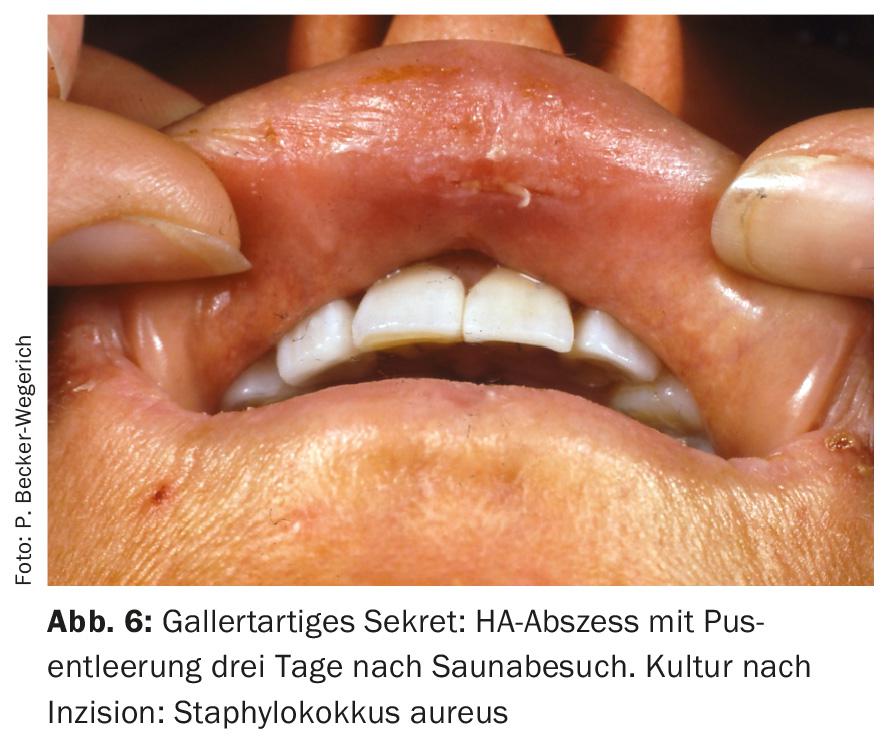
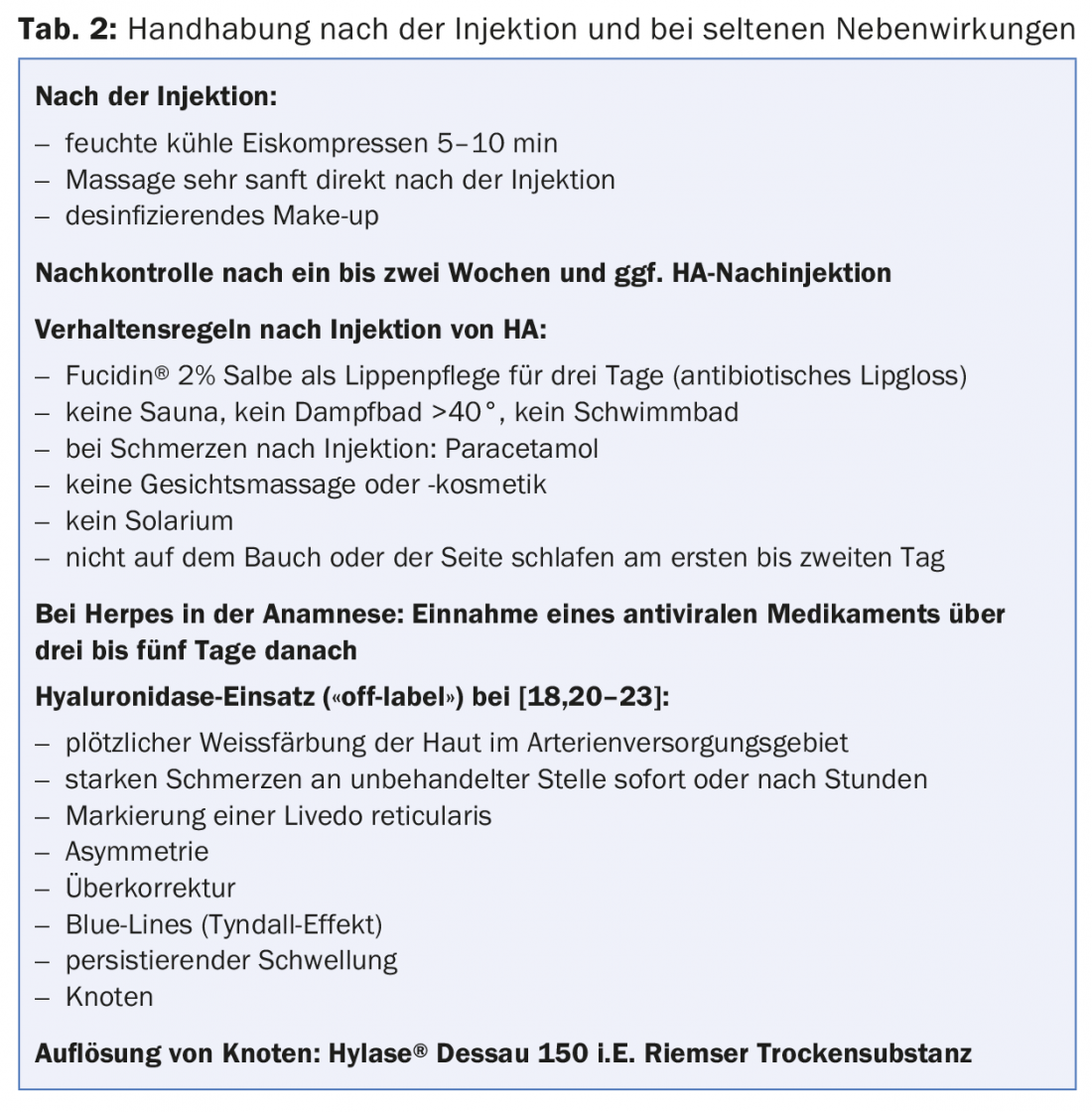
During and after lip enhancement with hyaluronic acid, occasional vasovagal syncope, pain or mild sensation of pressure, edema, erythema, hematoma, infection in the area of the injection sites, herpes thrust, Asymmetry (after local anesthetic infiltration block), overcorrection, blue lines (Tyndall effect), irregular contour or margins, and rarely pustules, papules, nodules, abscesses, and slippage of HA in deep stitched permanent makeup. (Fig. 6 and Tab. 2) [16,18].
Extremely rare possible persistent side effects include necrosis (including with residual scarring) and published isolated cases of blindness after vascular embolization or recurrent nodules (biofilm, BDDE allergy, type IV allergy such as foreign body granulomas) [16,17,19,20].
Both in the lip injection and in the surrounding area, too rapid injections with too much pressure and material should be avoided. Aspiration is recommended in areas of high vascularity. In case of sudden severe pain or headache, fading of the skin (“blanching” for more than ten minutes) or livedo drawing during and after the injection in the injection area or the surrounding area, the injection should be stopped immediately. Immediately inject hyaluronidase hourly in this area and surrounding areas until vascularization is restored. Waiting more than four hours diminishes the complete revascularization opportunity. The attending physician should generally be available after each injection. Patient safety comes first.
In case of suspicion and signs of vascular embolus (embolism of the retina) resulting in blindness, high doses (there is no maximum) of retrobulbar hyaluronidase should be injected immediately, provided one is familiar with the technique. The patient must be transferred immediately to the nearest ophthalmology clinic. Within the first 90 minutes, treatment should have occurred to prevent irreversible complete blindness [18–21].
We recommend that patients with a history of severe anaphylaxis to hymenopteran venoms or who have experienced severe swelling after sting events be tested and have a bee-wasp RAST taken in advance [22]. A patient in our aesthetic consultation reacted immediately after hyaluronidase injections (Hylase® “Dessau” [Riemser Company]) with massive perioral and enoral edema without systemic involvement. The RAST for IGE antibodies against Hylase® “Dessau” was positive, the RAST for wasp was equally high positive (>100 KU/l). Thus, type I allergies to hyaluronidase should always be considered before use in aesthetic corrective treatment.
Adverse reactions must be reported immediately to the product manufacturing companies and forwarded to an adverse reaction registry. We advise you to have adequate liability insurance (report side effects there as well). Beginners should first treat simple lips with little aging with HA.
In general, it is recommended to perform proper education and to use HA products long proven by evidenced studies. Seamless post-injection patient care is recommended and also allows beginners to sleep better. Home or beauty salon treatments, which often do not provide medical follow-up, are on the rise. We recommend avoiding such treatment routes for your own safety.
Filler and Botulinum Toxin A (BTX-A)
The combination of filler and botulinum toxin A (BTX-A) prolongs the durability of the filler. If you don’t want fillers, you can also see an effect with BTX-A. BTX-A is a safe and effective technique that can be used as a primary off-label treatment for upper lip wrinkles. Together with fillers, BTX-A can visibly influence the results and lead to a longer lasting and satisfying effect [24,25].
Assessment of the entire musculature located around the lips at rest and in facial expression determines the off-label use of BTX-A in these regions. Rare weakening of the mouth closure, whistling weakness, asymmetries or swallowing difficulties, which can very rarely occur with co-treatment of the platysma, must be included in the explanation in writing. Singers or actors should not be injected or should be restrained with lowest doses.
BTX-A microdoses into the upper dermis of the upper and lower lip do not weaken mobility, but affect vertical wrinkle regression and promote volume increase. Thus, function is preserved in the subcutaneous wheal technique via the upper fibers of the sphincter muscle. The depressor anguli oris muscle as well as the upper part of the platysma are responsible for pulling down the corners of the mouth with the lateral lip. The platysma is a mimic muscle that has a large facial expression component due to its insertion directly into the skin. BTX-A microinjections into this muscle (ligaments and mandibular junction) not only beautify the neck and lower facial contour, but soften the lateral cheek-chin wrinkles and lift the corner of the mouth. From the age of 50, we offer the combination of BTX-A with fillers (lifting the corners of the mouth using MD Codes™: Cheek-Reshape-Points and Marionette-Reshape-Points) and Thermage® or fractional lasers as an alternative for those who refuse more invasive lifting surgery.
Conflict of interest: This work was supported by graphical material and tables of the companies Galderma, Allergan and Merz, beyond that there are no further
Conflicts of Interest.
Acknowledgments: For providing the photographic material of the above-mentioned companies and Dr. Mauricio de Maio and for support PD Dr. S. Cotofana, Dr. Thorsten Walker, Dr. Siegfried Schmidt, Regine Raymond-Nachbauer and Marie Fritsche.
Literature:
- Raspaldo H, et al: Juvéderm volbella with lidocaine for lip and perioral enhancement: A prospective, randomized, controlled trial. Plast Reconstr Surg Global Open 2015; 3(3): e321.
- Raspaldo H, et al: Lip and perioral enhancement: A 12- Month Prosective Randomized, Controlled Study. J Drugs Dematol 2015; 14(12): 1444-1452.
- Cartier H, et al: Perioral Rejuvenation With a Range of Customized Hyaluronic Acid Fillers: Efficacy and Safety Over Six Months With a Specific Focus on the Lips. Journal of Drugs in Dermatology 2012; 11(1 Suppl): s17-26.
- Becker-Wegerich PM: Interview: Rejuvenation of the lips. This way you create a harmonious result. The German Dermatologist 2015; 63(10): 6
- Carruthers A, et al: A validated lip fullness garding Scale. Dermatol Surg 2008; 34(Suppl 2): 161-166.
- Kane MA, et al: Validation of a lip fullness scale for assesment of lip augmentation. Plast Reconstr Surg 2012; 129(5): 822e-828e.
- De Maio M: The 8-point-lip-reshape: Topographical anatomy. In: De Maio M: Unlocking the code to facial revitalization: A step-by-step approach to using injectables. Brazil 2015.
- Belhaouri Lakhdar: Enhancing and restoring youth to lips with hyaluronic acid. European Journal of Aesthetic Plastic Surgery 2012; 1: 1-148.
- Penna V, et al: Classification of the aging lips. Aesth Plast Surg 2015 Feb; 39(1): 1-7.
- Swift A, et al: BeautiPHIcation: A global approach to facial Beauty. Clin Plast Surg 2011; 38: 347-377.
- Hexsel D, et al: Double-blind, randomized, controlled clinical trial to compare safety and efficacy of a metallic cannula with that of a standard needle for soft tissue augmentation of the nasolabial folds. Dermatol Surg 2012 Feb; 38(2): 207-214.
- Solish N, Swift A: An open-label, pilot study to assess the effectiveness and safety of hyaluronic acid gel in the restoration of soft tissue fullness of the lips. J Drugs Dermatol 2011; 10(2) :145-149.
- Redaelli A: Managing Lip Rhytides Combining Botulinum Toxin and Hyaluronic Acid. Prime-journal.com 2011. DOI: 10.1080/21598908.2011.628215.
- Jacono AA: A New Classification of Lip Zones to Customize Injectable Lip Augmentation. Arch Facial Plastic Surg 2008; 10(1): 25-29.
- Sarnof DS, Gotkin RH: Six steps to a perfect lip. J Drugs Dermatol 2012; 11(9): 1081-1088.
- Rohrich RJ, et al: Soft Tissue Filler Complications: The important role of biofilms. Plast Reconstr Surg 2010; 125(4): 1250-1256.
- Bachmann F, et al: Adverse reactions caused by consecutive injections of different fillers in the same facial region: risk assessment based on the results from the Injectable Filler Safety study. J Eur Acad Dermatol Venereol 2011; 25: 902-912.
- Becker-Wegerich P: New indications for Hyaluronic acid of the NASHATM-gel-generation – highlights from aestetical dermatology in clinical daily rotine. J Dtsch Dermatol Ges 2008; 6(Suppl 3): S3-20.
- Bachmann F, et al: Consecutively injected fillers in the same region do not pose an increased risk for adverse reactions. J Eur Acad Dermatol Venereol 2011; 25: 737-738.
- Funt D, Pavicic T: Dermal fillers in aesthetics: an overview of adverse events and treatments approaches. Clinical Cosmetic and Investigation Dermatology 2013; 6: 295-316.
- Kim DW, et al: Vascular Complications of HA fillers and the role of hyaluronidase in management. Journal of Plastic Reconstructive Aesthetic Surgery 2011; 64: 1590-1595.
- Beleznay K, et al: Avoiding and Treating Blindness from Fillers: A Review of the World Literature. Dermatol Surg 2015; 41(10): 1097-1117.
- Kim MS, et al: Allergic reaction to hyaluronidase use after hyaluronic acid filler injection. J Cosmet Laser Ther 2015; 17(5): 283-285.
- Becker-Wegerich P: Wrinkle treatment with botulinum toxin A and special indications. In: Krutmann J, Diepgen T, Billmann-Krutmann C (Eds.): Skin Aging: Principles, Prevention, Therapy. Springer 2008; 75-100. DOI: 10.1007/978-3-540-76821-0_6.
- Kreyden OP, et al: Swiss Croup of Esthetic Dermatology and Skincare. The satisfied patient in aesthetic dermatology. Consensus work on patient satisfaction in treatment with botulinum toxin A. Dermatologist 2015; 66: 131-136.
DERMATOLOGIE PRAXIS 2016; 26(4): 26-30









