
Adequate symptomatic local treatment can optimally promote wound healing. In addition, a reduction in the risk of complications and an improvement in the quality of life can be achieved. The M.O.I.S.T treatment regimen, based on the T.I.M.E concept, is now considered the standard of modern local therapy. Special consideration is given to the restoration of oxygen balance and the use of specific wound therapeutics for poorly healing wounds.
A chronic wound is a symptom of several underlying conditions. The most common are diabetic foot ulcers, decubitus ulcers or leg ulcers. In parallel with the treatment of the underlying diseases, symptomatic local therapy oriented to the phases of wound healing is essential. Among other things, infection status, exudate volumes, but also individual patient wishes must be taken into account. An important treatment goal is to transform the microenvironment of the chronic wound into one that is conducive to the healing process. The elements of local wound treatment summarized under the acronym “M.O.I.S.T.” are a further development of the T.I.M.E concept first published about twenty years ago and widely used internationally. It is now recognized by many professional societies, including the umbrella organization for the German-speaking region Wund-DACH, as the standard of modern local therapy, explained Prof. Dr. med. Joachim Dissemond, Clinic for Dermatology, Venereology and Allergology, University Hospital Essen (D) [1,2].
The most important at a glance
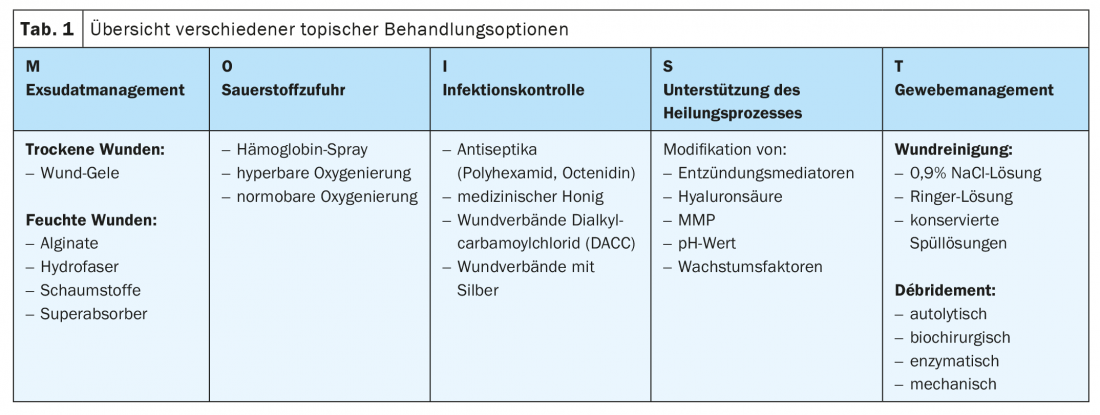
The factors of the T.I.M.E concept described as T (“Tissue”, tissue/wound bed), I (“Infection”, infection) and M (“Moisture”, exudate) are still timely and important. The letter ‘E’ was originally used to describe “epidermis” and later the wound margin (“Edge”). Since there have been many innovations in the past decade, an expansion to include additional components has been made. With O (“Oxygen Balance”) and S (“Support”), two modern new therapy aspects are taken into account in the M.O.I.S.T concept (Tab. 1) [2,3]. The following is an overview of the individual factors:
M – Moisture Balance (exudate management): Optimal moisture balance has been considered the gold standard for the treatment of chronic wounds for years. The wound environment should be neither too moist nor too dry. Dry wounds can be moistened with hydrogels. For wounds with high exudate volumes, the use of superabsorbents has proven effective.
O – Oxygen Balance (oxygenation): Hypoxia plays a crucial role in the pathophysiology of chronic wounds. If measures such as revascularization and compression therapy are not sufficient, treatment options that restore oxygen balance can be used. Dressings, hemoglobin spray, and other procedures are available for this purpose.
I – Infection Control: All antimicrobial strategies are subsumed under infection control. The indication for systemic antibiotic therapy is usually limited to systemic infections. Antiseptics such as polihexanide, octenidine or wound dressings containing silver, for example, are used for infection prophylaxis, eradication of multi-resistant germs or treatment of local infections.
S – Support (support of the healing process): If the measures used so far are not sufficient to heal wounds, specific wound therapeutics can be used temporarily, which actively intervene in the disturbed wound healing process. These include, for example, the modulation of matrix metalloproteinases (MMPs), ph levels or growth factors.
T – Tissue Management: This includes all measures of wound conditioning (e.g. by means of wound products, biosurgery or physical aids such as negative pressure, electricity, plasma or ultrasound). Depending on the method, debridement, wound cleansing, granulation or re-epithelialization can be supported.
The respective treatment steps are to be carried out in the sense of a phase-adapted procedure. Wound cleansing and debridement are performed first, followed by stimulation of granulation tissue growth and promotion of epithelialization [4]. Especially in chronic wounds of the lower extremities and edema, compression therapy has an important role in the treatment/prophylaxis of recurrence [5].
|
Oxygen is essential for the healing process of chronic wounds In most wounds, there is a lack of oxygen, also known as hypoxia. This often results in significantly slowed wound healing [14]. The European Wound Management Association (EMWA) has also pointed out the necessity of oxygen supply for wound healing in a document on oxygen treatment (“Use of oxygen therapies in wound healing “) [12]. O2 is essential for the wound healing process with regard to the formation of new vessels and connective tissue [12]. The oxygen supply to the wound is further compromised in patients with chronic wounds by underlying conditions such as diabetes or chronic venous insufficiency associated with decreased blood flow. |
Specific wound therapeutics such as MMP & co.
These are very innovative products with varying levels of evidence, said Prof. Dissemond. For this reason, it is difficult at the present time to make a clear recommendation for the indication of a particular procedure. But for poorly healing wounds, he said, it is worth considering these methods on a trial basis. In addition to matrix metalloproteinases (MMPs), the relevant armamentarium includes inflammation mediators (TNF-α inhibitors, β-glucan), growth factors (PDGF-BB, TGF-β), hyaluronic acid and chitosan. The best known method is the inhibition of MMP – for example, by sucrose octasulfate [6]. In a 2018 study in patients with diabetic foot ulcers published in the Lancet, treatment with dressings containing sucrose octasulfate showed a significantly higher wound closure rate compared to a control group with dressings without this substance [2,7]. The study included 240 adult diabetic patients with a noninfectious diabetic foot ulcer (>1 cm2, grade IC or IIC*). Study participants were randomized to local therapy with vs. without sucrose octasulfate (n=126, n=114). After a period of 20 weeks, wound closure manifested in 60 patients (48%) in the sucrose octasulfate group and in 34 patients (30%) in the control group (adjusted odds ratio 2.60, 95% CI 1.43-4.73; p=0.002).
* Categorization according to the University of Texas Wound Classification System (UT) for foot ulcers.
|
Integrated care: standardized wound documentation of the SAfW In 2020, the Swiss Society for Wound Management (SAfW) published a systematically derived documentation of wound care in view of the planned electronic patient dossier [13]. This is intended to contribute to quality improvement in integrated wound care and scientific studies. The 7 parameters to which 27 variables are assigned are: Patient master data, wound history, wound status, other wound-related diagnostics, therapy, and patient-reported outcomes (PROMs). The “Recommendation standardized documentation” is available for download free of charge on the SAfW homepage. |
Oxygen balance: promote O2 supply
The healing of a wound is accompanied by increased oxygen demand [11,13] (box). As approaches to improve oxygen supply in patients with chronic poorly healing wounds, there are various innovative methods such as oxygen transport in wounds by O2 transporters [2,8]. A hemoglobin spray can be used according to Strohal et al. used for the treatment of chronic wounds such as diabetic foot ulcers, secondary healing surgical wounds, leg ulcers, burns up to grade IIb and decubitus ulcers [9,10]. Another method is therapy with light oxygen overpressure. The application is limited to the area of the wound and the wound surroundings. Namely, an oxygen concentrator generates pure oxygen from the air and delivers it to the wound through positive pressure into a cuff attached to the wound area [9]. Another method mentioned is therapy with continuous oxygen gassing without overpressure. The principle of operation is that pure oxygen flows continuously onto the wound surface without additional pressure. O2 is generated from the circulating air and moistened before being delivered directly to the wound surface via a diffuser. Often, the oxygen diffuser is combined with an O2-tight dressing to further promote the wound healing process. This treatment option is also intended primarily for chronic wounds that prove refractory to standard treatment and, according to Iniitative Chronische Wunden e.V. 2016, is particularly suitable for diabetic foot ulcers, leg ulcers, trauma wounds and postoperative injuries with wound healing disorders [9,11].
Congress: Wound Congress Nuremberg
Literature:
- Protz K, Timm JH: Modern wound care, 9th edition, 2019, Urban & Fischer Verlag/Elsevier.
- Dissemond J: Modern wound therapy according to the MOIST concept. Prof. Dr. med. Joachim Dissemond, Nuremberg Wound Congress, 02.-03.12.2021
- Initiative Chronische Wunden e.V: Standards/Definitions, www.icwunden.de/wundwissen/standardsdefinitionen/m, (last accessed 04.01.2022).
- Dabiri G, Damstetter E, Phillips T: Adv Wound Care (New Rochelle) 2016; 5(1): 32-41.
- Dissemond J: Modern management of chronic wounds, Der Hautarzt, Issue 8/2021, 20/07/2021.
- Dissemond J, et al: Sucrose octasulfate-evidence in the treatment of chronic wounds. Dermatologist 2020; 71: 791-801.
- Edmonds M, et al: Sucrose octasulfate dressing versus control dressing in patients with neuroischaemic diabetic foot ulcers (Explorer): an international, multicentre, double-blind, randomised, controlled trial. Lancet Diabetes Endocrinol 2018; 6: 186-196.
- Gottrup F, et al: Use of Oxygen Therapies in Wound Healing. Journal of wound care 2017; 26(Sup5): S1-s43
- Mayr C: The importance of oxygen in wounds, 2017, wundmanagement-tirol.at, (last accessed 04.01.2022).
- Strohal R, et al: Expert consensus on practice-relevant aspects of wound therapy with a hemoglobin spray. Wound Management 5/2016, 276-284.
- Chronic Wounds Initiative: Oxygen deficiency and chronic wounds. Information Guide. Quedlinburg: 2016.
- EMWA: Negative pressure wound therapy, Journal of Wound Care 2017, 26(5), https:// ewma.org (last accessed 04.01.2022).
- Swiss Society for Wound Management (SAfW): Recommendations standardized documentation. SAfW Umbrella Company 10/2020, www.safw.ch/images/safw/dokumente/Standard_Wunddoku_Schweiz.pdf (last accessed Jan. 04, 2022).
- Federal Joint Committee, www.g-ba.de/downloads/40-268-4943/2018-04-19_AM-RL_Abschnitt%20P_Verbandmittel_ZD.pdf (last accessed Jan. 04, 2022).
- Dissemond J: M.O.I.S.T. – a concept for the local therapy of chronic wounds. Clinical Letter. JDDG 2017; 15(4): 443-445.
DERMATOLOGIE PRAXIS 2022; 32(1): 34-36









