Multiple myeloma, the pathological proliferation of immunoglobulins in the bone marrow, is still considered incurable. However, highly effective drugs prolong survival – in rare cases up to 20 years.
Only a few people know what the term “multiple myeloma” means – this is how Florin Rupper, President of the Myeloma Contact Group Switzerland (MKgS), characterized the state of public knowledge. Education and networking of those affected is necessary. In this context, Prof. Dr. med. Christoph Driessen, Chief Physician of the Clinic for Medical Oncology and Hematology of the Cantonal Hospital St. Gallen, provided information about the rare cancer at a press conference.
Very heterogeneous and etiologically unclear
250 people in Switzerland are newly diagnosed with multiple myeloma every year. According to the Swiss Cancer Registry, there are currently around 2500 people affected. Multiple myeloma is the product of a monoclonal proliferation of immunoglobulins in the bone marrow. The malignant disease manifests itself genetically and clinically in a very heterogeneous manner. About a quarter of all myeloma patients are asymptomatic. If symptoms occur, they range from bone pain (60%, mostly in the trunk skeleton) and fatigue (40%, often anemia-related) to weight loss, frequent infections, hypercalcemia, and decreased renal function and foamy urine (proteinuria, albuminuria) [1]. Although associations with genetic factors, radiation or chemical exposure, autoimmune diseases, other plasma cell diseases, and viral infections are suspected, the pathogenesis remains unclear.

The precursor of multiple myeloma is always a monoclonal gammopathy of unknown significance (MGUS). This is a common, benign proliferation of a plasma cell clone. It occurs with increasing frequency in old age: Around 10% of ninety-year-olds exhibit this change. In about 1% of affected individuals, MGUS degenerates into multiple myeloma. Again, the older the person, the more likely they are to develop multiple myeloma. But exceptions prove the rule, as the case of a 49-year-old patient shows (box).

Pain due to bone resorption
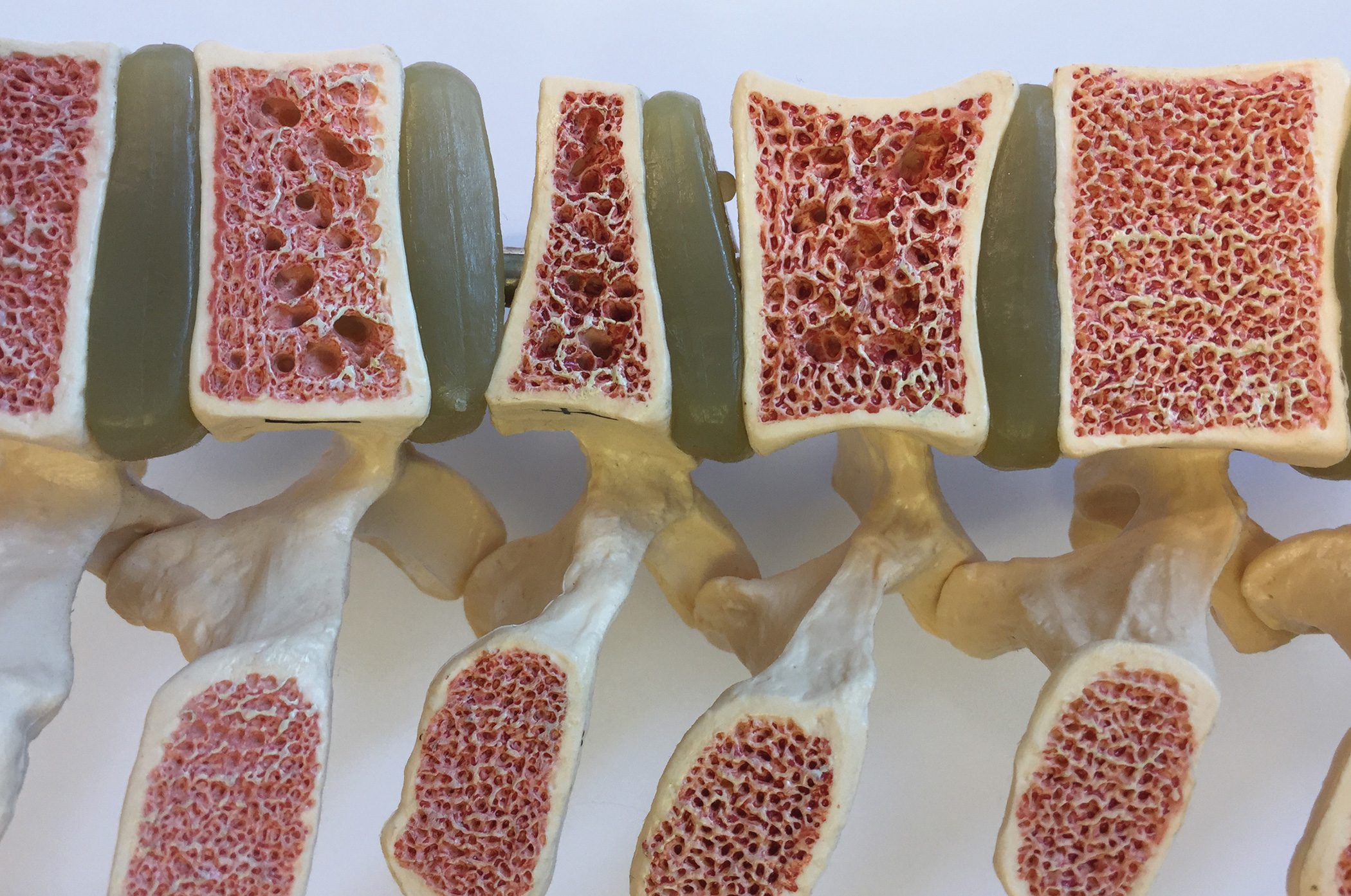
The growth of immunoglobulins in the bone marrow displaces blood and immune cells, leading to anemia, fatigue, and a tendency to infection and bleeding. Moreover, myeloma cells activate bone resorption (Fig. 1). The consequences are severe osteoporosis, fractures, associated pain and fatigue, and even confusion. Deposition of protein chains in the kidneys leads to renal failure. A manifestation also outside the bone marrow entails pain and loss of strength.

If myeloma is suspected, in addition to a medical history and physical examination, various laboratory tests are performed to determine blood levels of various proteins (paraprotein, beta-2-microglobulin, creatinine, albumin) and electrolytes. A blood count provides information about the leukocytes. Changes in the bones are detected by CT, MRI and, if necessary, PET. The bone marrow is examined with the help of a bone marrow biopsy.
New drugs improve survival
According to the current state of research, there is no cure for multiple myeloma. Treatment of symptomatic myeloma patients is primarily aimed at achieving the best possible remission with rapid control of symptoms and myeloma-related complications. This is because multiple myeloma is a progressive disease that progresses in relapses. The long-term goal is to prolong the progression-free period and thus overall survival [1].
A retrospective Real World multicenter study based on medical records of 5000 myeloma patients provided informative data on the courses [2]. After diagnosis, the patient receives six months of therapy, which is followed by six months of maintenance therapy. On average, patients then spend ten months without therapy before the disease returns. However, with each therapy escalation, the therapy-free interval shrinks. “The time without therapy is becoming shorter and shorter,” summarizes Prof. Driessen, “and the proportion of patients who receive the next therapy is also becoming smaller and smaller.
However, with the development of new drugs, survival has improved significantly. The mean value is just over six years. Data from eastern Switzerland prove this. Prof. Driessen is therefore hopeful: “This is one of the cancers with the fastest improving prognosis due to these new drugs.” He said there are more “survivors,” patients who live longer with the disease. However, according to Prof. Driessen, the great challenge lies in the initial diagnosis: How can one distinguish at diagnosis which patient will survive longer – 10 to 20 years – and who will die of the disease within a year? Genetic analyses provide clues.
Therapeutic applications include local therapies, radiotherapies, chemotherapies, corticosteroids, and novel approaches such as immunomodulators (e.g., thalidomide, lenalidomide, pomalidomide), proteasome inhibitors (e.g., bortezomib, carfilzomib, ixazomib), and – more recently – monoclonal antibodies (e.g., deratumumab, elotuzumab). “For the first time, we now have very effective immunotherapies that can work for a long time and are significantly better tolerated than chemo,” says Prof. Driessen, but immediately points out a problematic fact: Currently, patients have to wait for years before the cost-intensive therapy is approved by health insurance.
Source: Press conference MKgS, Zurich
Literature:
- German Society for Hematology and Medical Oncology: Guideline Multiple Myeloma. ICD10: C90.0. Recommendations of the professional society for the diagnosis and therapy of hematological and oncological diseases. Status 2018.
- Yong K, et al: Multiple myeloma: patient outcomes in real-world practice. Br J Haematol. 2016; 175(2): 252-264.
HAUSARZT PRAXIS 2019; 14(6): 28-29 (published 5/24/19, ahead of print).
InFo ONCOLOGY & HEMATOLOGY 2019; 7(5): 20-21.