
Folic acid is important for cell growth and division and prevents neural tube defects. Optimal folate status is especially central for women of childbearing age. Therefore, folic acid supplementation is recommended if pregnancy is planned.
Folic acid is now used worldwide as a supplement, a voluntary food additive, and as a mandatory fortification of a staple food. This is the chemically produced form of the vitamin known as folate, also called vitamin B9. Folates naturally occurring in plant and animal foods consist of a pteridine and p-aminobenzoic acid ring with two to nine glutamate residues attached to the carboxyl end (polyglutamates). Folic acid contains only one glutamic acid residue. Of all folate-active compounds, it is the most stable form with the highest oxidation state and is almost completely absorbed as a pure substance (tablet, capsules) on an empty stomach. Folates, on the other hand, are sensitive to light, heat and oxygen. During absorption, the polyglutamate chain must be degraded first, which is why folates are absorbed only 50-60% [1]. For this reason, today the requirement value for folate/folic acid is given in folate equivalents [FÄ]. The requirement values according to the D-A-CH recommendations are compiled in table 1.
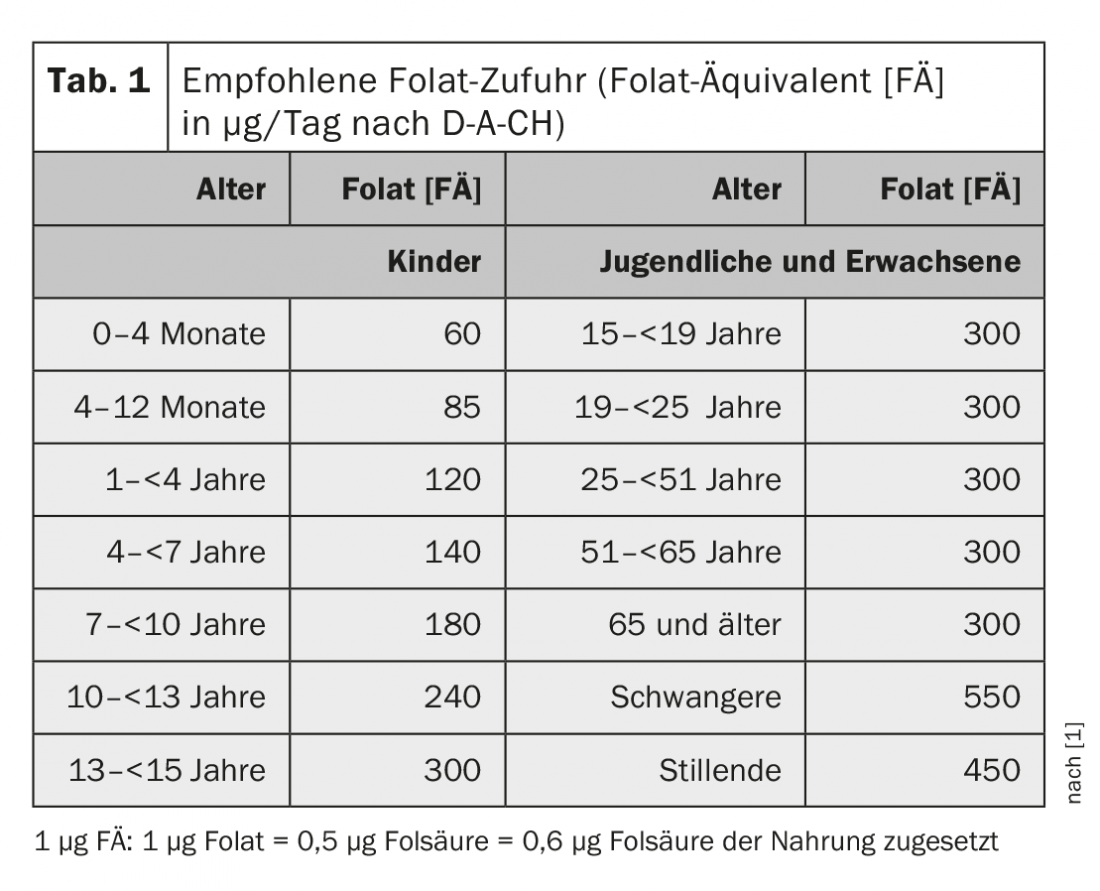
Guideline values regarding folic acid requirement
In the human organism, folate is subject to various transport and metabolic processes and regulations. The active form is 5-methyltetrahydrofolate (5-MTHF). Folate can be measured in serum/plasma and in erythrocytes (storage form). Serum concentration indicates the level of folate in the blood, but says nothing about tissue reserves. Concentrations <7 nmol/l folate are considered deficiency, those <10 nmol/l as subclinical deficiency with risk of elevated homocysteine. Folate concentration in erythrocytes is an indicator of longer-term supply (norm: 450-1130 nmol/l). Concentrations <340 nmol/l indicate a deficiency, values >906 nmol/l are necessary for possible prophylaxis of a neural tube defect [2].
The food sources rich in folate are liver (>200 µg/100 g) and raw greens such as kale, peas, spinach and salads (140-190 µg/100 g). So far, there are only few data available on the supply of the Swiss population. The intake level is calculated based on the consumption of the corresponding foods and was 295 µg/day per person in recent years [3]. In a recent study of erythrocyte folate levels in pregnant women, only 47% achieved a level desirable for open back prevention. 19.8% of nonpregnant women of reproductive age had folate deficiency [4].
Folates are important for cell function, growth and division. They are involved in the formation of purines and pyrimidines and thus in DNA and RNA synthesis. Together with other B vitamins, they regulate homocysteine concentrations and, as methyl (C1) group donors, play an important role (also epigenetically) in DNA methylation. In this function, folates can influence the activity of genes and thus contribute to the prophylaxis of malformations or diseases. Whether long-term folic acid undersupply increases the risk of chronic disease can only be estimated by observational studies of folate intake comparing undersupplied with normally supplemented individuals or comparing equivalent populations before or after mandatory fortification. Intervention studies, as often called for by experts, are not feasible for these questions today.
Folic acid as a supplement
Folic acid as a single substance or as part of a multivitamin can be used in the form of tablets, capsules, powder or effervescent tablets in the following situations:
- As a drug to treat folic acid deficiency at a dose of 1 mg/5 mg/10 mg/day
- To improve the intake in case of increased need (single preparation or multivitamin) in special situations such as pregnancy, lactation, in certain diseases (e.g. diseases of the gastrointestinal tract) or in certain therapies (Bactrim®, methotrexate), smoking and alcohol excess or physical and mental stress. The dose is 200-600 µg/day.
- For prevention of neural tube defects min. 400 (up to max. 800) µg/day min. One month (better three) before conception and in the first twelve weeks of pregnancy.
- To optimize the daily requirement, usually 200 µg daily (equivalent to 340-400 FÄ), supplied mainly through fortified foods.
- Folate in the form of active 5-MTHF in humans with polymorphisms of 5,10-methylenetetrahydrofolate reductase (MTHFR).
- Folic acid in the form of folinic acid (Leucovorin®), 15 mg as a tablet or 10 mg in the solution for injection, especially in sick (i.v.-fed) patients
Folic acid as a dietary supplement
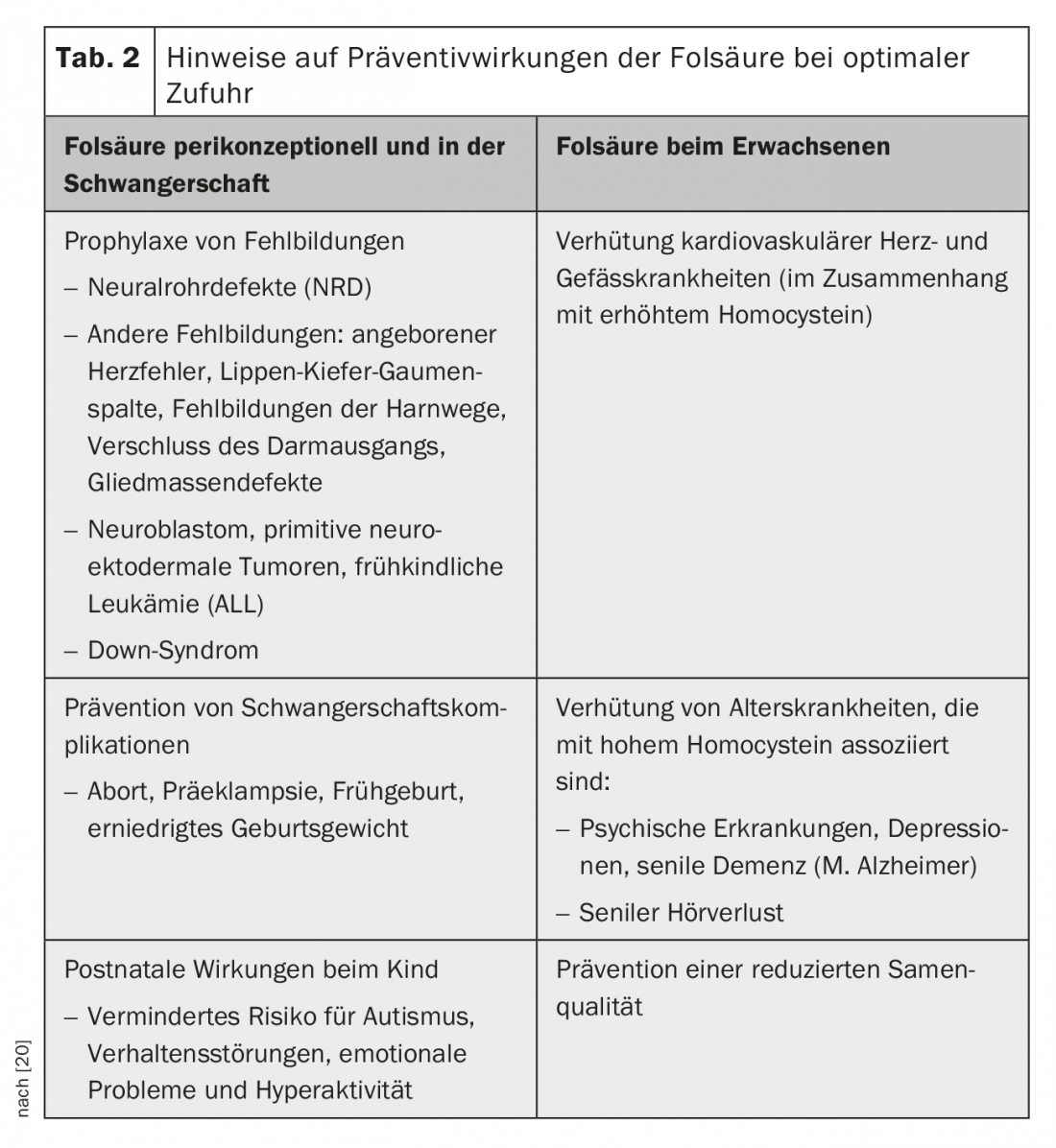
Dietary supplements allow food manufacturers to supplement their products to offer consumers important micronutrients in addition to food. Since folic acid was recognized as an important element in the prevention of neural tube defects, this application has expanded. In Switzerland, the Folic Acid Foundation (www.stiftung-folsaeure.ch) has helped to publicize the preventive effects of folic acid. Table 2 is to be understood in such a way that an insufficient folate supply is seen as a risk factor for the diseases mentioned. Of particular importance are the pre- and periconceptional phases, pregnancy and the first years of child development, where the epigenetic influence of folic acid is strongest. However, folic acid also plays a role in later life and old age, especially in situations where elevated homocysteine levels are involved (e.g., dementia) [5,6].
Add folic acid compulsorily?
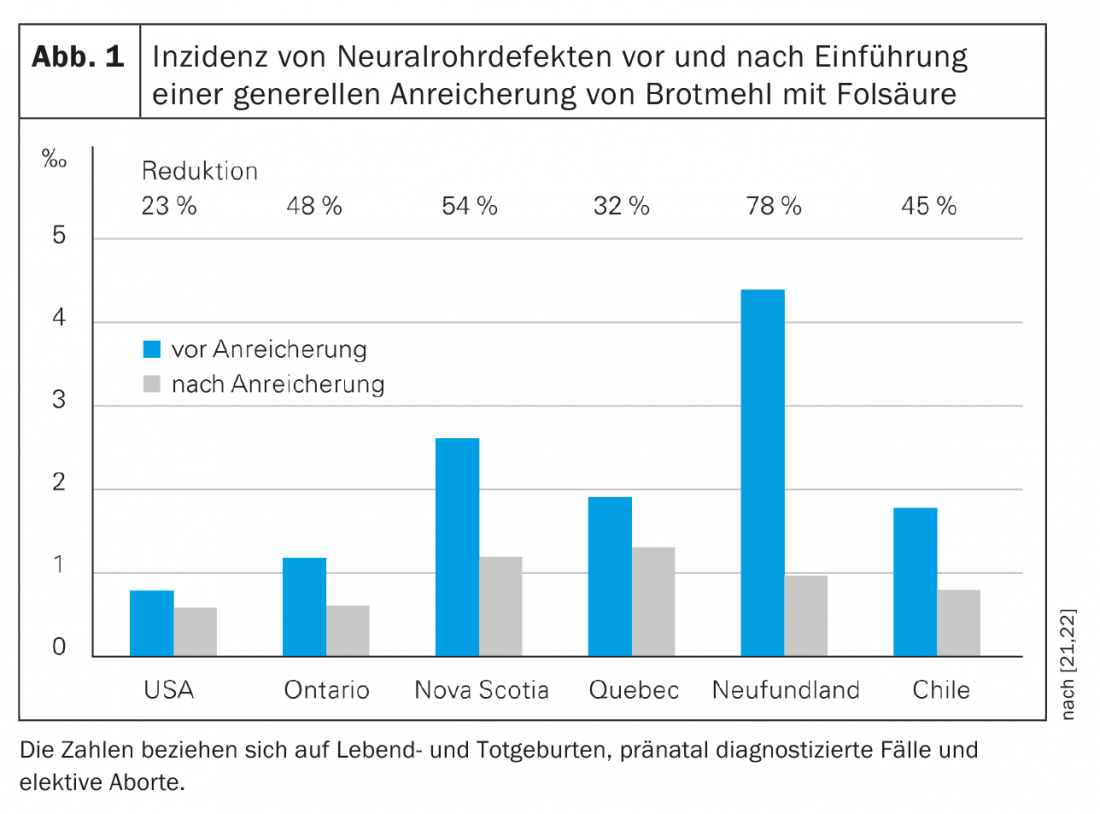
In more than 80 countries, flour or rice are compulsorily fortified with folic acid, which reduces the risk of neural tube defects by 30-70% [7] (Fig. 1) . Apart from Malta, no European country currently fortifies a staple food with folic acid on a mandatory basis. In Switzerland, flour fortification is carried out only on a voluntary basis (so far in at least five mills). An official proposal by the Federal Nutrition Commission (FEC) in 2002 for mandatory fortification of flour with folic acid was criticized by consumer organizations as a coercive measure and declared by a legal opinion to be incompatible with the current law [8]. England is the first Western European country that now wants to introduce mandatory enrichment to prevent uncontrolled enrichment [9].
Food supplementation is regulated by law. No more than 600 µg/day (800 µg/day for women of childbearing potential, pregnant women up to the twelfth week of pregnancy) should be taken. a maximum daily dose of 300 µg can be added [10,11]. However, the problem arises here that the daily intake can be exceeded by the consumption of various fortified foods, as was found in a German market analysis for children [12].
News from the research
About 300 scientific articles on folic acid are published annually. Results of some of this new work (2016 to 2018) will be briefly presented below.
Cost savings through prevention: the prevention of spina bifida through the administration of folic acid is also associated with cost savings. A 2015 study found that the direct cost to a patient was $791000. Fortification of flour with folic acid costs $0.15-1 per ton of flour, totaling $4 million. If the assumption holds that spina bifida can be prevented in 767 live-born children in one year as a result, up to $603 million could be saved per year [13].
Heart health: the same could be true for the prevention of congenital heart defects. Maternal folic acid supplementation before conception conferred a reduced risk of congenital heart defects of 58% overall (=OR 0.42; 95% CI 0.21-0.86), with some differences between individual heart defects: OR 0.37 for malformations of the great vessels, OR 0.34 for atrial septal defect. Low dietary folate intake and no supplementation during pregnancy was associated with an approximately twofold increased risk of heart defects [14].
Influence on the brain: In children, there is a slight age-related thinning of the cerebral cortex thickness in the frontal and temperal lobes after birth until early adolescence. Delay of this process is associated with higher intelligence, and acceleration with schizophrenia and autism. American authors have now used MRI in a retrospective study to examine the cerebral cortex thickness in 8- to 18-year-olds in three cohorts – in each case before the fortification of flour with folic acid (before July 1, 1996), in the transition phase (until June 30, 1998) and after the introduction (from July 1, 1998). In the adjusted collective, they found a significant association of higher cerebral cortex thickness with prenatal folic acid exposure in a total of 292 MRIs with comparable conditions in the three groups (97/96/99), and thus a reduced risk for psychosis spectrum symptoms. This finding is consistent with European studies that found lower brain volume in young children and later behavioral problems with inadequate periconceptional folic acid intake. This was explained by epigenetic modification of genes regulating cortical development or mitigating the influence of toxic influences [15].
A meta-analysis with a total of 4514 autism patients describes the association of maternal folic acid supplementation during pregnancy with the risk for autism. Folic acid supplementation reduced the risk by 23% (RR 0.77; 95% CI 0.64-0.93) [16]. Another prospective study of 1250 mother-infant pairs found a U-shaped relationship between maternal multivitamin supplementation and infant risk for autism, in which both low and very high plasma folic acid and B12 levels were associated with increased risk [17].
C1 metabolism and cancer risk: A dysbalance in C1 metabolism is associated with certain types of cancer. A Chinese research group reported in a meta-analysis on the association of the four vitamins involved in C1 metabolism (B2, B6, folic acid, and B12) with the risk of developing esophageal cancer. 26 Studies included 6404 cases of esophageal Ca and 504 550 controls. This involved determining the OR for the highest vs. lowest levels of each vitamin in relation to esophageal Ca. This showed that a folic acid increase of 100 µg/day reduced the risk by 12% (95% CI 9-14%). For vitamin B6, an increase of 1 mg/day reduced the risk by 16% (95% CI 11-20%). In contrast, increasing vitamin B12 by 1 µg/day increased the risk of esophageal Ca by 2% (95% CI 0-3%), especially in Europe and the United States. The authors therefore suggest that geographic and histologic differences exist [18].
Pregnancy complication preeclampsia: Preeclampsia occurs in 3-5% of all pregnancies and can endanger the life of mother and child. Epidemiological studies suggested that high doses of vitamins, including folic acid, may prevent the risk. Therefore, a randomized clinical trial was initiated in 2011 at 70 centers in five countries. 2464 women at high risk of preeclampsia took either 4 mg of folic acid or a placebo daily from the eighth to the 16th week of gestation until delivery (however, the placebo group was also allowed to take a vitamin supplement including folic acid up to 1.1 mg). The endpoint of the study was preeclampsia beginning at 20 SSW. Of the 1144 women in the intervention group, 14.8% had preeclampsia, compared with only 13.5% in the control group (1117 women). So not all studies show a positive result. However, this study involved therapeutic use rather than long-term preventive use. The treatment was well tolerated and without side effects [19].
Summary
Folic acid continues to have an important role as a supplement in the prevention of neural tube defects. Every woman of childbearing age should maintain optimal folate status to provide the best possible protection for her child in the event of an unexpected pregnancy. In case of pregnancy planning, the additional intake of at least 400 (up to max. 800) µg folic acid, preferably in the form of a multivitamin, is indicated one to three months before conception and in the first twelve SSW. Folic acid is significant for cell division, growth and epigenetics through its mode of action in DNA synthesis, DNA repair and DNA methylation. This explains their preventive importance for some chronic diseases – not only in children, but also in adults.
Take-Home Messages
- Folic acid is important for cell growth and cell division.
- It plays an important role as a methyl donor for homocysteine metabolism as well as DNA and RNA synthesis and methylation – and thus epigenetically.
- Folic acid prevents neural tube defects. Pregnant women should therefore take at least three months beforehand and during the first twelve weeks of pregnancy. Take 400 µg of folic acid in addition to a balanced diet.
- There is evidence that folic acid also has other preventive effects in children and adults.
- The intake of folates is too low or borderline for a part of the population, esp. in the case of a polymorphism in the enzyme MTHFR (in 15% of the population). Therefore, a targeted intake is recommended for optimal supply.
Literature:
- German Society for Nutrition, Austrian Society for Nutrition, Swiss Society for Nutrition (eds.): Reference Values for Nutrient Intakes, 1st edition, 5th correction version. Frankfurt: Umschau/Braus-Verlag 2013: 127-152.
- Daly LE, et al: Folate levels and neural tube defects. Implications for prevention. JAMA 1995; 274(21): 1996-1702.
- Federal Office of Public Health (FOPH) (ed.): Sechster Schweizerischer Ernährungsbericht. Bern 2012: 90-91.
- Herter-Aeberli I: Personal communication.
- Li W, et al: Folic Acid Alters Methylation Profile of JAK-STAT and Long-Term Depression Signaling Pathway in Alzheimer’s Disease Models. Mol Neurobiol 2016; 53(9): 6545-6556.
- Bender A, Hagan KE, Kingston N: The association of folate and depression: A meta-analysis. J Psychiatr Res 2017; 95: 9-18.
- Food Fortification Initiative (FFI): March 2017 Newsletter. http://ffinetwork.org/about/stay_informed/newsletters/2017Q1.html, last accessed Jan. 21, 2019.
- Baerlocher K, et al: Folic acid: expert report of the Swiss Federal Commission on Nutrition for the prophylaxis of neural tube defects. Bern: BAG 2002: 43-47.
- Drbyos: fortification with folic acid to prevent birth defects. News World 2018. https://www.nach-welt.com/gesundheit/anreicherung-mit-folsaure-um-geburtsfehler-zu-vermeiden, last accessed Jan. 21, 2019.
- EDI: Ordinance of the EDI on Food Supplements of December 16, 2016, as of May 1, 2018.
- EDI: Ordinance of the EDI on the Addition of Vitamins, Minerals and Other Substances to Foods of December 16, 2016, as of June 5, 2018.
- Kersting M, Alexy U: Vitamin and mineral supplements for the use of children on the German market: products, nutrients, dosages. Ann Nutr Metab 2000; 44(3): 125-128.
- Grosse SD, et al: Retrospective Assessment of Cost Savings from Prevention: Folic Acid Fortification and Spina Bifida in the U.S. AM J Prev Med 2016; 50(5 Suppl 1): 74-80.
- Mao B, et al: Maternal folic acid supplementation and dietary folate intake and congenital heart defects. PLoS ONE 2017; 12(11): e0187996.
- Eryilmaz H, et al: Association of Prenatal Exposure to Population-Wide Folic Acid Fortification With Altered Cerebral Cortex Maturation in Youth. JAMA Psychiatry 2017; 75(9): 918-928.
- Wang M, et al: The association between maternal use of folic acid supplements during pregnancy and risk of autism spectrum disorders in children: a meta-ananlysis. Molecular Autism 2017; 8: 51.
- Raghavan R, et al: Maternal Multivitamin Intake, Plasma Folate and Vitamin B12 Levels and Autism Spectrum Disorder Risk in Offspring. Peadiatr Perinat Epidemiol 2017; 32(1): 100-111.
- Qiang Y, et al: Intake of Dietary One-Carbon Metabolism-Related B Vitamins and the Risk of Esophageal Cancer: A Dose-Response Meta-Analysis. Nutrients 2018; 10(7): E835.
- Wu WS, et al: Effect of high dose folic acid supplementation in pregnancy on pre-eclampsia (FACT): double blind, phase III, randomised controlled, international, multicentre trial. BMJ 2018; 362: k3478.
- Baerlocher K: The multiple health benefits of adequate folic acid intake. Family Practice 2014; 9: 28-34.
- Tönz O: Folic acid. Voluntary addition to various foods or mandatory fortification of a staple food. Ther Umsch 2007; 64: 171-176.
- Eichholzer M, Tönz O, Zimmermann R: Folic acid: a public-health challenge. Lancet 2006; 367: 1352-1361.
FAMILY PRACTICE 2019; 14(2): 6-9









