
In April, birch and ash pollen dominate the pollen count in this country. Up to 15% of the population suffer from rhinitis and asthma in the spring. An occasion to draw attention to the increasing clinical importance of ash pollen for spring pollinosis.
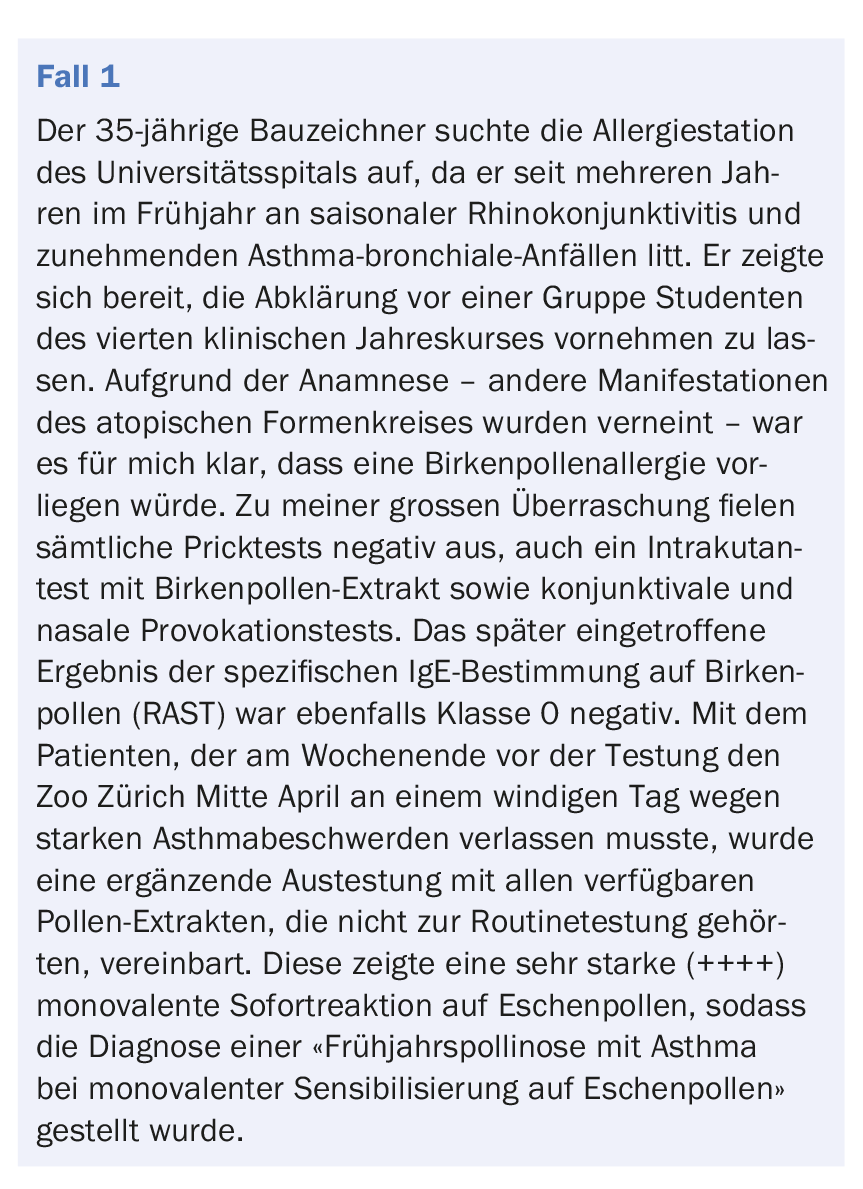
In the month in which this issue of Dermatology Practice is published, birch and ash pollen dominate the pollen count in our region. During the spring months of March/April, up to 15% of the population suffers from rhinitis and asthma, and pollinosis symptoms during this period were attributed to birch pollen (BP, Betula sp.) more than 25 years ago [1]. Case 1 provided an opportunity to draw attention to the increasing clinical importance of ash pollen (EP, Fraxinus sp.) in spring pollinosis.
This observation led to the inclusion of ash pollen (EP) in routine testing. In the context of a doctoral thesis by Prof. Peter Schmid-Grendelmeier, at that time assistant physician at the allergy ward, the frequency of sensitization to ash pollen and its clinical relevance was investigated [2].
Ash pollen is now part of routine allergy testing
From July to December 1991, data from 623 pollinosis patients (mean age 29 years, 52% of whom were male) were analyzed. 88% of patients reported symptoms in the early summer months. In the prick skin test, sensitization to grass and rye pollen (71%) was found most frequently, followed by pollen from alder (58%), ash (51%), birch, hazel (47% each), and mugwort (35%). 417 patients (67%) were classified as spring pollinitis with rhinoconjunctivitis based on their symptoms in March and April, 31% additionally with asthma, of whom 57% were sensitized to BP and 56% to EP. 118 patients (19%) were positive exclusively for tree pollen. Monovalent sensitization to ash pollen was detected in 15 patients. Nasal provocation tests in 50 patients were positive with EP in 72% and with BP in 80%.
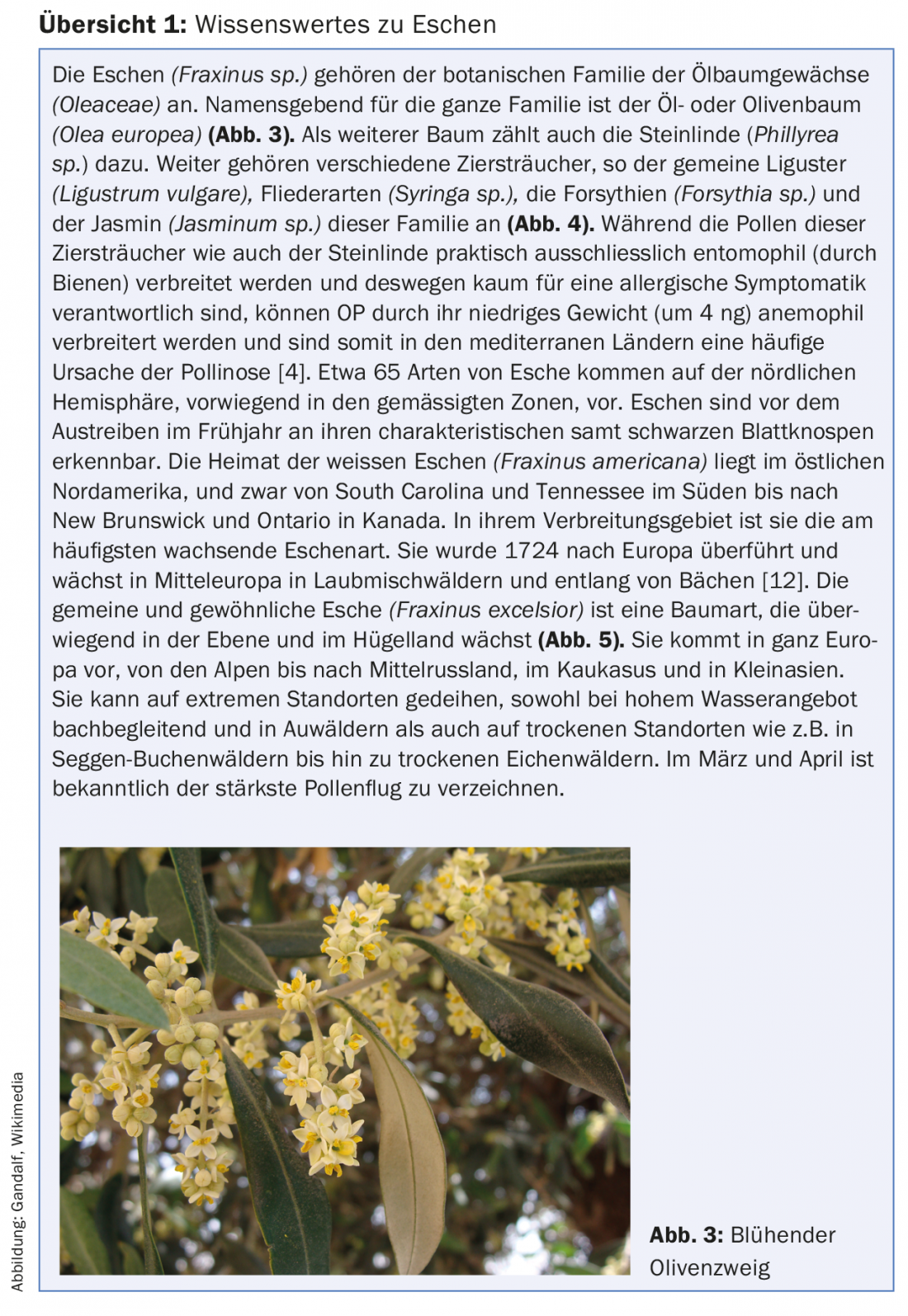
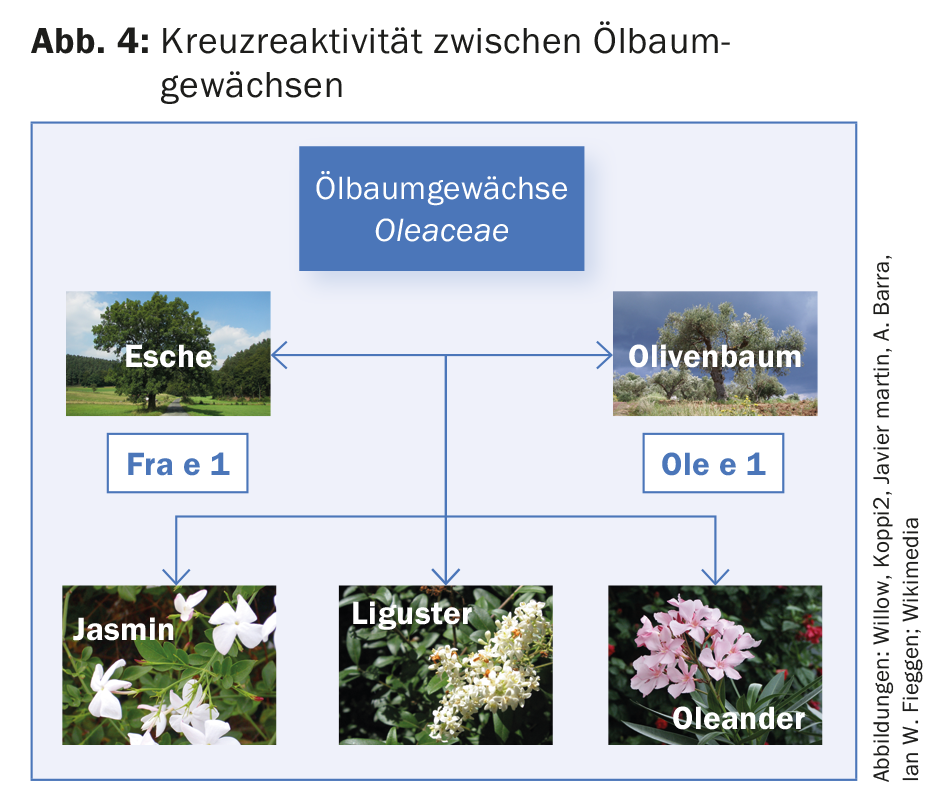
Thus, it could be shown that spring pollinosis is of increasing importance in northern Switzerland, but also in the southern part of Ticino and in certain areas of central Europe – as a result of the increased tree pollen count in recent years [3,4]. EP must be considered in diagnostics – monovalent sensitization occurs – and in specific immunotherapy [2,5,6]. Ash trees belong to the botanical family of the olive family (Oleaceae), so there is strong cross-reactivity within this family [7]. As a consequence of this cross-reactivity of EP with olive pollen (OP), especially to Olea europea, an EP-allergic person can suffer from a respiratory allergy during a stay in the Mediterranean region in late winter/spring or a Southerner with OP-allergy can suffer from a respiratory allergy when settling in Switzerland during the pollen flight of EP.
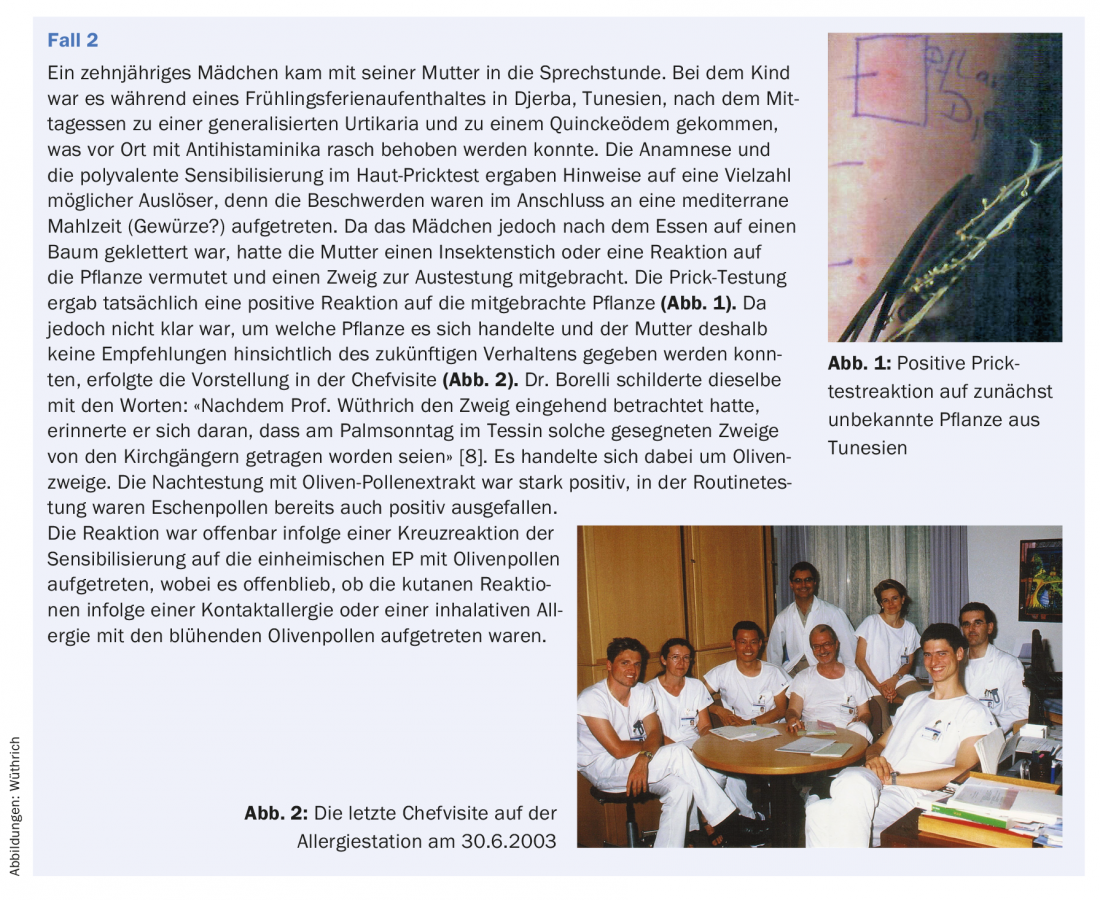
Olive branches are distributed to churchgoers on Palm Sunday in Ticino
In an essay on the occasion of my retirement from the University Hospital in June 2003, Dr. Siegfried Borelli recalls a case presentation in the daily chief rounds in the allergy ward (case 2) [8].
Not all ash trees are the same
Based on three clinical observations (cases 3-5) , I was able to show in 2006 – at that time practicing at the Zollikerberg Hospital – that the CAP routinely offered for in vitro IgE diagnostics of the species Fraxinus americana (t15) has a lower sensitivity than that of the native ash Fraxinus excelsior (t25) [9]. As a conclusion, I postulated that standardized extracts of Fraxinus excelsior should be used for both in vivo and in vitro testing as well as for specific immunotherapy [9].
On cross-reactivity within the olive family
Although there is naturally a strong cross-reactivity between Fraxinus americana (CAP t15, Pharmacia) and Fraxinus excelsior (CAP t25) (overview 1) [12], the above case observations show that apparently certain allergenic epitopes must be present in Fraxinus excelsior that are absent in Fraxinus americana. In two cases (cases 3 and 4) , CAP t15 was false-negative and in the fifth case, where there was also a clinically significant olive pollen allergy, it was weak. The commercial prick test solution is made from the common ash tree. Due to this fact, Pharmacia Diagnostica (Sweden) also offers a regular ImmunoCAP for Fraxinus excelsior (t25) with CE label as an addition to the allergen product range since mid-2006, which is more specific for our region [13].
From conventional pollen extracts to the main marker allergens
Conventional pollen allergen extracts – like those of EP – contain mixtures of allergenic components, some of which have been detected. The main allergen in EPs is Fra e 1, a glycoprotein that has a very high cross-reactivity due to the high sequential match with the main allergen of OP Ole e 1 (a glycoprotein with a sequence of 145 amino acids) [14]. Therefore, ole e 1 is considered a marker allergen not only for OP but also for EP [15] and SIT with olive pollen extract is recommended if EP extracts are not available for SIT [15,16]. Currently, standardized EP or OP allergen extracts for SIT or also for sublingual immunotherapy (SLIT) are not registered in Switzerland and therefore not automatically eligible for health insurance. Nevertheless, the allergist has the possibility to order corresponding products from the distribution company as Formula magistralis. In the interest of the patient, a request for a cost credit agreement for this product should be submitted to the respective insurance company in advance. Distributors may not officially name and advertise such.

The following allergens have to be ordered from the respective distributors as a Formula magistralis formulation for SIT or SLIT (with cost credit):
- Olive pollen for Allergovit® (Allergopharma)
- Ash (Fraxinus excelsior) and olive pollen as native allergens/tyrosine (Bencard)
- Olive pollen as allergoid/tyrosine (Bencard)
- Olive pollen as an allergen/tyrosine/MPL adjuvant (Bencard).
- Ash (or ash/birch) as Phostal® or
- Alyostal® (Stallergenes)
- Olives for Oralvac®
- Ash (Fraxinus excelsior) or birch/ash 50/50 and olive for Staloral® 300
ALK currently does not market any ash or olive pollen preparations in Switzerland.
Literature:
- Helbling A, Leuschner R, Wüthrich B: Pollinosis. IV: Which pollens should be tested in allergy practice? Results of the determination of allergenic pollen in the air of Zurich in 1981-1984 considering threshold concentrations. Schweiz Med Wochenschr 1985; 115: 1150-1159.
- Schmid-Grendelmeier P: On the significance of ash pollen allergy in spring pollinosis. Clinical-anamnestic investigations based on skin tests and provocation tests as well as in-vitro investigations for cross-reactivity with birch pollen by means of RAST inhibition, CRIE and Western blot inhibition. Med Diss Zurich 1993.
- Wüthrich B, et al: Pollinosis. III. pollen calendar of Zurich with the allergologically most important pollen species. Air pollen determinations in the Zurich area during the years 1977, 1978 and 1979 in the framework of the study of “Groupe international de recherches aéropalynologiques appliquées”. Schweiz Med Wochenschr 1983; 113: 170-183.
- Wüthrich B, Peeters A: Allergenic pollen and pollinosis in Switzerland. In: D’Amato G, et al. (Eds.): Allergenic Pollen and Pollinosis in Europe. Blackwell Scientific Publications 1991; 197-202.
- Schmid P, Peeters A, Wüthrich B: L’allergie au pollen de frêne existe en Suisse, nous l’avons rencontrée. Rev fr Allergol 1992; 32: 139-140.
- Schmid-Grendelmeier P, et al: On the significance of ash pollen allergy. Allergology 1994; 17: 535-542.
- Wahl R, et al: In vitro investigation of cross-re activity between birch and ash pollen allergen extracts. J Allergy Clin Immunol 1996; 98: 99-106.
- Borelli S: A Ticino in Zurich. hautnah schweiz 2003; 4: 30.
- Wüthrich B: Ash is not ash. Allergology 2006; 29: 231-235.
- Wüthrich B, Hofer T: Food allergy: the “celery-mugwort-spice syndrome”. Association with mango fruit allergy? Dtsch Med Wochenschr 1984; 109: 981-986.
- Wüthrich B: Memories of an allergist: Nocturnal asthma attacks instead of “dreamy and cozy sleep”. Dermatology Practice 2016; 26(6): 46-50.
- Niederberger V, et al.: The allergen profile of ash (Fraxinus excelsior) pollen: cross-reactivity with allergen from various plant species. Clin Exp Allergy 2002; 32: 933-941.
- Vaith P: Preliminary information on the allergen ash. Sweden Diagnostics AB. Personal communication on 12/21/2005.
- Twaroch TE, et al: Carrier-bound, nonallergenic Ole e 1 peptides for vaccination against olive pollen allergy. J Allergy Clin Immunol 2011; 128: 178-184.e7.
- Palomares O, et al: The major allergen of olive pollen Ole e 1 is a diagnostic marker for sensitization to Oleaceae. Int Arch Allergy Immunol 2006; 141: 110-118.
- Imhof K, et al: Ash pollen allergy: reliable detection of sensitization by IgE to ole e 1. Allergo Journal 2014; 23(3): 18-23.
DERMATOLOGIE PRAXIS 2018; 28(2): 30-35
DERMATOLOGIE PRAXIS 2018 Special Edition (Anniversary Issue), Prof. Brunello Wüthrich









