The phosphodiesterase 4 (PDE4) inhibitor, which has been approved for this indication since last year, persistently reduces both the number of oral ulcers and associated pain. Overall, apremilast treatment is associated with a significant improvement in the quality of life of patients with Behçet’s syndrome. However, the differential diagnostic differentiation from aphthoses of other causes sometimes proves challenging. At this year’s SGDV annual meeting, two experts summarized the current state of knowledge and their clinical experience in an interdisciplinary symposium.
Behçet’s disease (synonym: Behçet’s syndrome) is a progressive vasculitis that can lead to severe multisystemic complications if left untreated. Almost all patients experience recurrent, painful oral ulcers during the course of the disease, which are associated with a reduced quality of life [1]. Prof. Dr. med. Peter Villiger, Rheumatologist, Monbijou Medical Center, Bern and Prof. Dr. med. Nikhil Yawalkar, Deputy Medical Director, Bern. Chief of Dermatology, Inselspital Bern, spoke at the SGDV Annual Congress on the epidemiology, clinical features and differential diagnosis of this rare disease and presented current facts on apremilast (Otezla®) – the first and so far only system therapy available in Switzerland for the treatment of oral aphthae in Behçet’s disease(box) [2].*
*Specifically related to the label of the drugs, as of June 2020. Full Indication Text: Otezla® is indicated for the treatment of persistent oral ulcers associated with Behçet’s disease in adult patients who have had an inadequate response to topical therapy [2].
M. Behçet is widely distributed along the Silk Road
Behçet’s disease is most common from the Mediterranean to China, Prof. Villiger said. For example, in Turkey, the prevalence is 370 per 100 000 inhabitants [1], while the corresponding values in Germany are 2.26-4.87 [3]. In Switzerland, the prevalence is estimated at 4.03 per 100 000 population [4]. This is the result of the extrapolation of a Bern study with 60 Behçet patients. Among them, immigrants from high-prevalence countries were significantly more likely to be affected, at 19.54%. The causes of Behçet’s disease are unknown. (Auto-)immunological and viral or bacterial triggers are thought to be involved and an association with the human leukocyte antigen B51 allele (HLAB51) is suspected.
Oral ulcers as the most common manifestation of Behçet’s syndrome.
In a cohort study of 428 patients, oral ulcers were present in 100% of study participants, 95% suffered from genital ulcers, and 83% were affected by papulopustular lesions. Because oral aphthosis can have numerous other causes, a “diagnostic delay” often occurs. In an analysis published in 2019, the diagnostic latency from the onset of oral ulcers to diagnostic classification as Behçet’s disease was a median of eight years, Prof. Villiger noted [4]. In the International Criteria for Behçet’s Syndrome (ICBD) classification system, the presence of the following symptoms is evaluated using a point system(Table 1): Oral aphthae, genital aphthae, skin lesions, ocular symptoms, neurological symptoms, vascular manifestations, positive pathergy test [5]. Prof. Yawalkar elaborated on some main symptoms [1]:
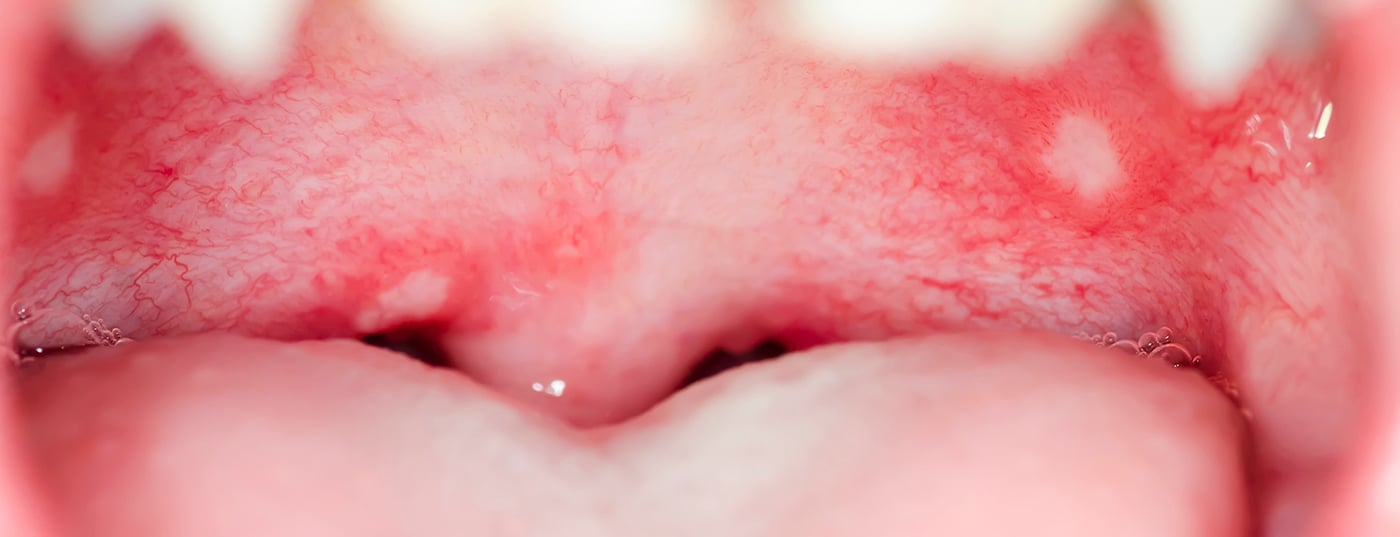
- In most Behçet’s patients, oral ulcers are the first to manifest. These are recurrent, painful and often multiple, irregularly shaped aphthae of varying diameters. The buccal mucosa, tongue, soft palate or oropharynx are frequently affected. Large lesions sometimes scar.
- Genital ulcers in Behçet’s disease are also recurrent, usually larger and painful aphthous lesions with a sharply demarcated ulcer margin and a punched-out appearance. The risk for scarring is high. In males, there is usually involvement of the scrotum. In females, the labial region is often affected, occasionally the vagina and perineum.
- Skin lesions occur in 50-80% of Behçet’s disease patients: inflammatory papulopustular lesions, pseudofolliculitis, erythemanodosum, Sweet’s syndrome- or P. gangrenosum-like lesions, or extragenital ulcers or cutaneous vasculitic lesions, respectively [1,6].


-
In 33-62% of Behçet’s patients there is a positive pathergy finding, characterized by the formation of a papule/pustule of a diameter of 2 mm within 24-48 hours. A skin prick (3 punctures) with 20-24 gauge needles can be used to perform the test [1,6].
Differential diagnostic differentiation from RAS
Differentiating between oral ulcers in Behçet’s disease and chronic recurrent aphthosis stomatitis (RAS) can be difficult, said Prof. Yawalkar. RAS is a diagnosis of exclusion when no underlying systemic disease has been identified. In this context, chronic recurrent aphthae occur in three clinically morphologic manifestations [7].
- Minor-type oral aphthae (diameter <1 cm): these account for 80-90% of all recurrent aphthae and usually heal spontaneously after 7-14 days, usually without scarring. The mucosa in the region of the lip and cheek mucosa or the anterior region of the floor of the mouth are frequently affected.
- Large oral aphthae of the major (Sutton) type (1-3 cm in diameter): are more painful, often more deeply indurated with a raised margin, whitish-yellowish pseudomembranes, and an erythematous yard. Typical localizations are lips, buccal mucosa, tongue, soft palate or oropharynx. They account for about 10% of benign recurrent aphthae, persist for 2-6 weeks, rarely longer. In about 64% of major-type aphthae, scars may develop after healing.
- Herpetiform aphthae (2-3 mm in diameter): are considered highly painful, are more common in females, and usually heal within 10 days. They can occur in numbers up to 100, confluent into larger erosive plaques, and usually heal without scarring. Any localization in the area of the mouth can be affected.
Behçet’s disease: significant relief of oral aphthosis by apremilast.
For the treatment of persistent Behçet’s disease-associated oral ulcers in adult patients who have not responded adequately to topical therapy, a systemic therapy option, apremilast (Otezla®), has been available in Switzerland for the first time since last year [2]. This treatment option, enshrined in the European League Against Rheumatism (EULAR) guideline, provides a stable decrease in the lesion number of oral ulcers while reducing pain [8]. The approval extension of apremilast is based in part on data from the randomized, placebo-controlled phase III RELIEF trial of 207 patients with Behcet’s disease [9]:
- Treatment with 30 mg of apremilast twice daily resulted in a significant reduction in the number of oral ulcers at week 12 (AUC†) 129.5 vs. 221.1; p<0.0001) [9,10]. This is of great clinical relevance, said Prof. Villiger. The rapid onset of action of apremilast should also be emphasized: the full clinical effect of the treatment manifested itself after only 1-2 weeks. Approximately half of those affected by Behçet’s disease (56.7%) showed complete healing of oral ulcers after 12 weeks under Otezla® [9]. After the former placebo arm was also treated with Otezla® in the subsequent follow-up until week 64, the number of ulcers was also reduced to an average of one in a few weeks, and the effect of the treatment was maintained until week 64(Fig. 1) [10]. After discontinuation of therapy, ulcers recurred [10].
- The most important secondary endpoint was the reduction in pain during the course of treatment. There was a massive reduction in pain in the verum group. This proved significant after only one week of apremilast treatment and persisted throughout the treatment period [10].
A complete treatment response was seen in up to more than half of apremilast-treated study participants during the 64-week treatment period [10]. In summary, apremilast is a very potent treatment option with a rapid and durable therapeutic effect with continued treatment, Prof. Villiger said. Standard dosing is known from psoriatic and psoriatic arthritis indications, and the beneficial safety profile is well documented [2,9].
This article was written with the financial support of Amgen Switzerland AG.
Literature:
Dermatology Practice; 2021 31(5): 22-24.










