Osteoporosis and osteomalacia are two metabolic bone diseases that reduce bone mass. In osteoporosis, there is a decrease in bone mass, but the ratio between bone mineralization and bone matrix is normal. In osteomalacia, the ratio of bone mineralization to bone matrix is decreased. An insufficient supply of calcium and vitamin D is one of the modifiable risk factors and can be remedied by appropriate supplementation.
Osteomalacia is due to decreased mineralization, usually due to marked vitamin D deficiency or impaired vitamin D metabolism. Possible causes are disorders that impair vitamin D absorption (e.g. celiac disease) or the intake of certain medications. Osteoporosis is characterized by low bone mass and microarchitectural changes in bone tissue. This results in an increase in bone fragility and a tendency to fracture.
Bone density decreases from the fourth decade of life onwards
Bone is remodeled and renewed throughout life; if this remodeling is not in balance, there is an age-correlated decrease in bone density. The causes of such an imbalance are multifactorial. Both the individual constitution, hormonal factors and lifestyle play a role. Osteoblasts (cells that form the bone matrix and mineralize the bone) and osteoclasts (cells that resorb the bone) are primarily regulated by parathyroid hormone, calcitonin, estrogen, and vitamin D. The highest bone mass is found in men and women around the age of 30, with men having a higher bone mass. After that, bone mass remains on a plateau for about 10 years, during which time new bone formation and bone resorption balance each other out. Subsequently, there is an annual bone loss of about 0.3-0.5%. With the onset of menopause, bone loss in women progresses at 3-5% per year for approximately 5-7 years before the rate of loss slows [1].
Calcium and vitamin D supply: influenceable risk factors
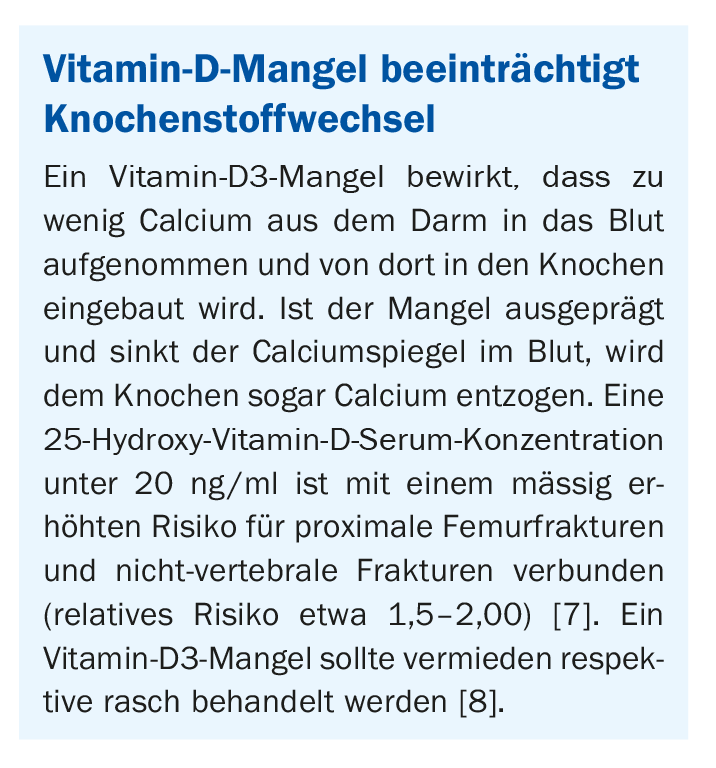
Extended periods of physical inactivity promote bone loss, because stress is necessary for bone growth. Low body mass index also predisposes to reduced bone mass. But insufficient intake of calcium, phosphorus, magnesium and vitamin D are also risk factors for bone loss. Vitamin D plays a central role in building and maintaining healthy bone by promoting the absorption of calcium from the intestine and the incorporation of calcium into bone (box) .
Unlike calcium, vitamin D is present in higher concentrations in only a few foods (e.g. salmon, cod liver oil, egg yolk, butter, mushrooms). The daily requirement is therefore only insufficiently covered by food. The greater part of the required vitamin D or precursors thereof is produced by sunlight in the skin and converted into a biologically active form in the liver and kidneys. For endogenous production of an adequate amount of vitamin D, 20 minutes of exposure 3 days per week with the forearms and face exposed is sufficient during the summer months [2]. In the winter months, vitamin D levels in the body often drop because the skin is covered by clothing and sunlight is so shallow that the skin cannot produce enough vitamin D.
Older people in particular are predisposed to vitamin D deficiency
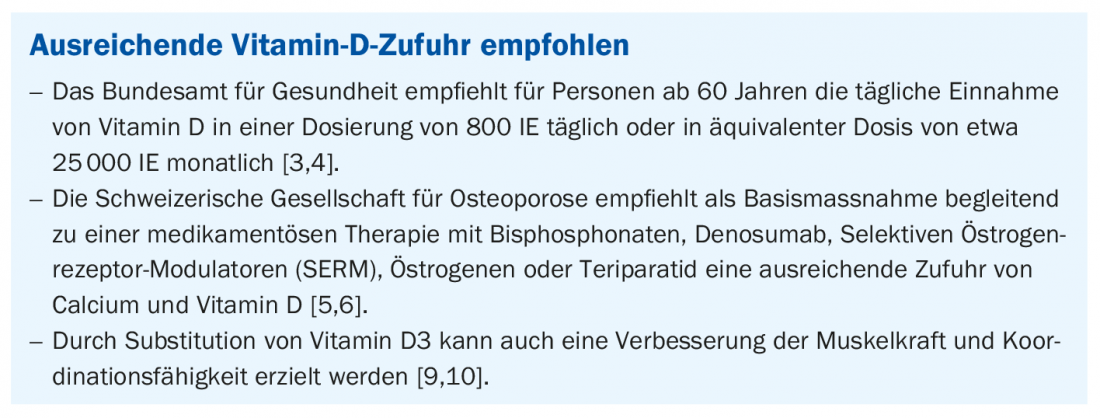
Vitamin D deficiency is generally more common in older people than in younger people: The vitamin D synthesis of aging skin decreases and older people are usually less often in the sun. Consequently, pronounced deficiencies are found relatively frequently in nursing home and old-age home residents. However, vitamin D3 deficiency is also common in people with dark skin tones, those who are overweight, and those who spend little time outdoors. Health authorities and professional societies recommend an adequate supply of vitamin D as a preventive and therapeutic measure with regard to osteoporosis (box). Viferol D3® 25 000 is indicated for the treatment of vitamin D deficiency in adults and adolescents 12 years of age and older, for the prophylaxis of vitamin D deficiency in adults over 60 years of age, and in adults with an identifiable risk of vitamin D deficiency disease due to malabsorption [11].
Literature:
- Bolster MB: Osteoporosis, www.msdmanuals.com, last modified Nov 2018 (last accessed 10/09/21).
- Rheumaliga Schweiz: Osteoporosis, leaflet, www.rheumaliga.ch (last accessed 10.09.2021).
- Federal Commission for Nutrition: Vitamin D deficiency: Evidence, safety, and recommendations for the Swiss Population. Expert report of the FCN. Zurich: Federal Office for Public Health, 2012.
- Bischoff-Ferrari HA, et al: JAMA Intern Med 2016; 176(2): 175-183.
- Ferrari S, et al: Swiss Med Wkly 2020, 150: w20352.
- Stute P, Meier C: Update osteoporosis. J Gynecol Endocrinol 2021, https://doi.org/10.1007/s41975-021-00181-4
- DVO: Guideline of the Umbrella Organization of the German-Speaking Scientific Osteological Societies e.V., 2017, www.awmf.org (last accessed Sept. 10, 2021).
- Bode LE, et al: J Am Med Dir Assoc 2020; 21(2): 164-171.
- Pfeifer M, et al: J Bone Miner Res. 2000; 15(6): 1113-1118.
- Pfeifer M et al: Osteoporos Int 2009; 20(2): 315-228.
- Technical information Viferol D3® 25’000, www.swissmedicinfo.ch (last accessed Sept. 10, 2021).
HAUSARZT PRAXIS 2021; 16(9): 46









