
Case report: The then 37-year-old physiotherapist had received a ball to the right temple while playing tennis during her vacation in Turkey. After a brief headache and throbbing in the left ear, severe dizziness and balance problems with inability to stand and walk occurred the following morning. She vomited several times and was admitted to a local hospital. There, imaging demonstrated a left PICA infarct due to vertebral dissection.
Primary therapy consisted of combined administration of Aspirin®, clopidogrel, and Clexane® (2.0 × 0.6 ml). After repatriation to our clinic, we confirmed persistent vertebral dissection on ultrasound and MRI (Fig. 1) and switched to Aspirin®, 100 mg daily, as monotherapy according to the current data and extension of the dissection to intradural.

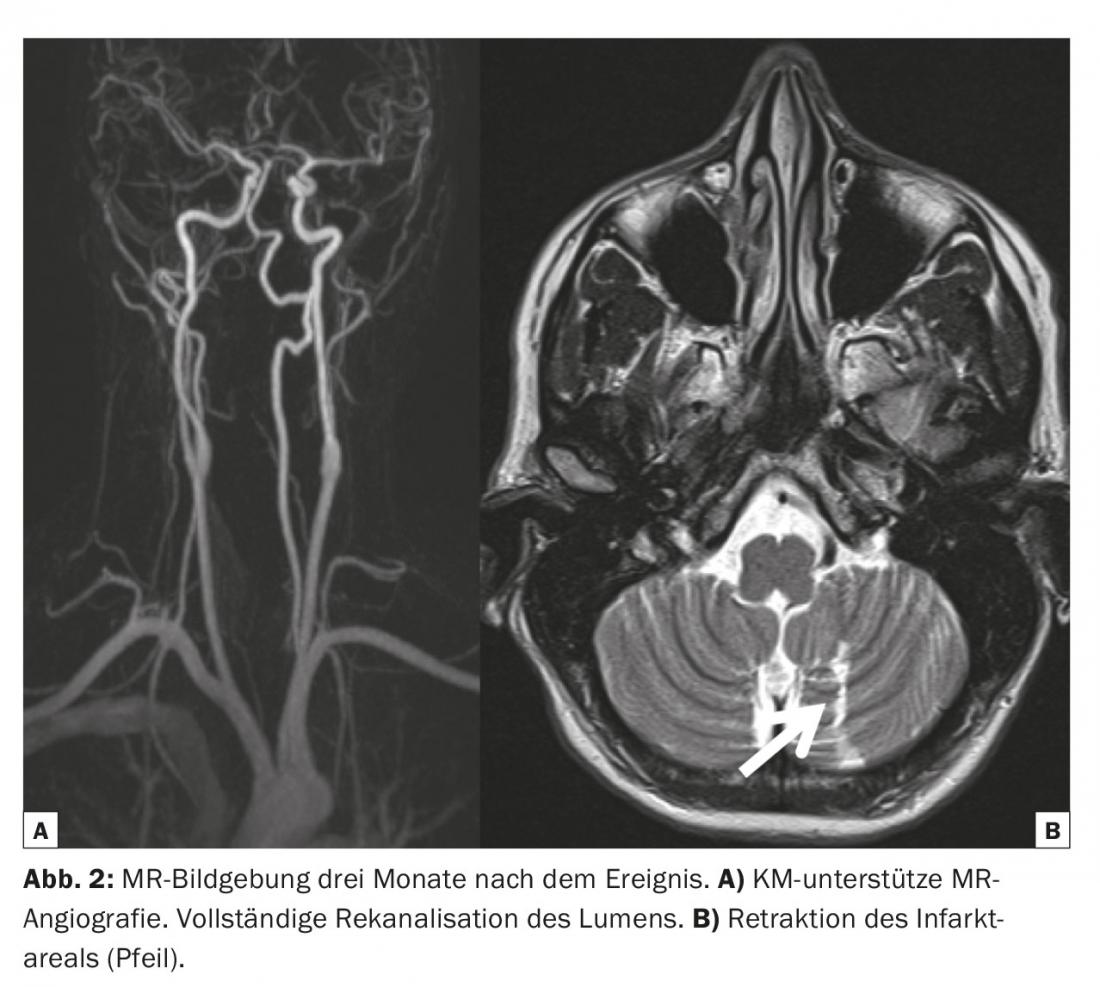
In addition, the patient received a low molecular weight heparin (Fragmin®) for thrombosis prophylaxis. After prompt transfer to neurological rehabilitation, the condition improved protractedly until complete freedom from symptoms. Follow-up checks by ultrasound and MRI confirmed complete recanalization of the vessel (Fig. 2). In the meantime, the patient has returned to work at 100 percent capacity and, apart from occasional attacks of dizziness in “stress situations”, is symptom-free.
Of note from the history is a right vertebral dissection sustained several years earlier after chiropractic maneuver, which was not detectable on current imaging. Neurologic symptoms or imaging signs of cerebral ischemia had not existed at that time.
Discussion: If even mild neurological symptoms, (dissection-typical) pain, and/or Horner’s syndrome (which had not been observed in our patient) occur after sudden, possibly jerky head movements – in our case report, a sudden reflexive head turn after tennis ball hit to the temple – then this must suggest a dissection of the carotid and/or vertebral arteries.
Various diagnostic modalities (CT, MRI, and ultrasound) are very good at documenting dissection or its hemodynamic effects in the acute phase and can provide noninvasive evidence of recanalization during follow-up visits. Meanwhile confirmed in the CADISS study [1], Aspirin® in monotherapy is the current therapy recommendation in secondary prophylaxis.
The course after dissections of the neck arteries is often more benign and the risk of recurrence is lower than in cerebral strokes of arteriosclerotic origin [2]. Although dissections may occur with exercise, this certainly does not translate into the “no sports” recommendation attributed to Winston Churchill.
Literature:
- CADISS trial investigators: Lancet Neurol 2015 Apr; 14(4): 361-367.
- Georgiadis D, et al: Neurology 2009; 72: 1810-1815.
InFo NEUROLOGY & PSYCHIATRY 2015; 13(5): 30-31.









