
Atrial fibrillation remains a common condition that increases with age. Nevertheless, the diagnosis is not infrequently due to chance. Guidelines therefore advocate opportunistic screening starting at age 65. Could this approach be purposeful? And what challenges must be overcome in pregnant patients with atrial fibrillation?
Atrial fibrillationis a relevant disease whose incidence increases with age. Up to 5% of the population suffer from the often symptomless disease. However, if left untreated, secondary complications may occur. Early diagnosis would therefore be desirable. Guidelines advocate opportunistic screening of all persons 65 years of age and older. In a worldwide study, this approach was shown to detect undetected AF in approximately 1.4% of cases studied. Various non-invasive methods are available for screening. These include, for example, smartwatches or other handheld devices. This means that a visit to the doctor’s office or hospital is no longer absolutely necessary. As a rule, this approach leads to good acceptance by those affected.
Sense or nonsense of systematic screening
A large-scale Swedish study assigned all people in a birth cohort to a systematic screening or control group. Over the two-week period, an ECG was written twice daily and recorded with a handheld device. In particular, in this study population, new cases of VCF were detected both in the ECG at baseline and in the first seven days of self-discharge. In these cases, anticoagulation was initiated. After an observation period of six years, the patients showed a significantly reduced risk of stroke, hemorrhage, embolism and mortality. A Danish study came to similar conclusions. Here, 32% of the subjects were diagnosed with atrial fibrillation. In the control group, only 12%. The risk of stroke was also reduced, although not significantly.
Researchers agreed that although a one-time opportunistic screening can detect persistent AF, the technology is not yet sophisticated enough to detect episodic fibrillation. In principle, systematic screening could become cost-effective after three years and save costs of about 1.8 million euros by preventing strokes and their hospitalization. Further analyses are currently underway to further elucidate the feasibility and viability of large-scale screening.
Arrhythmias during pregnancy
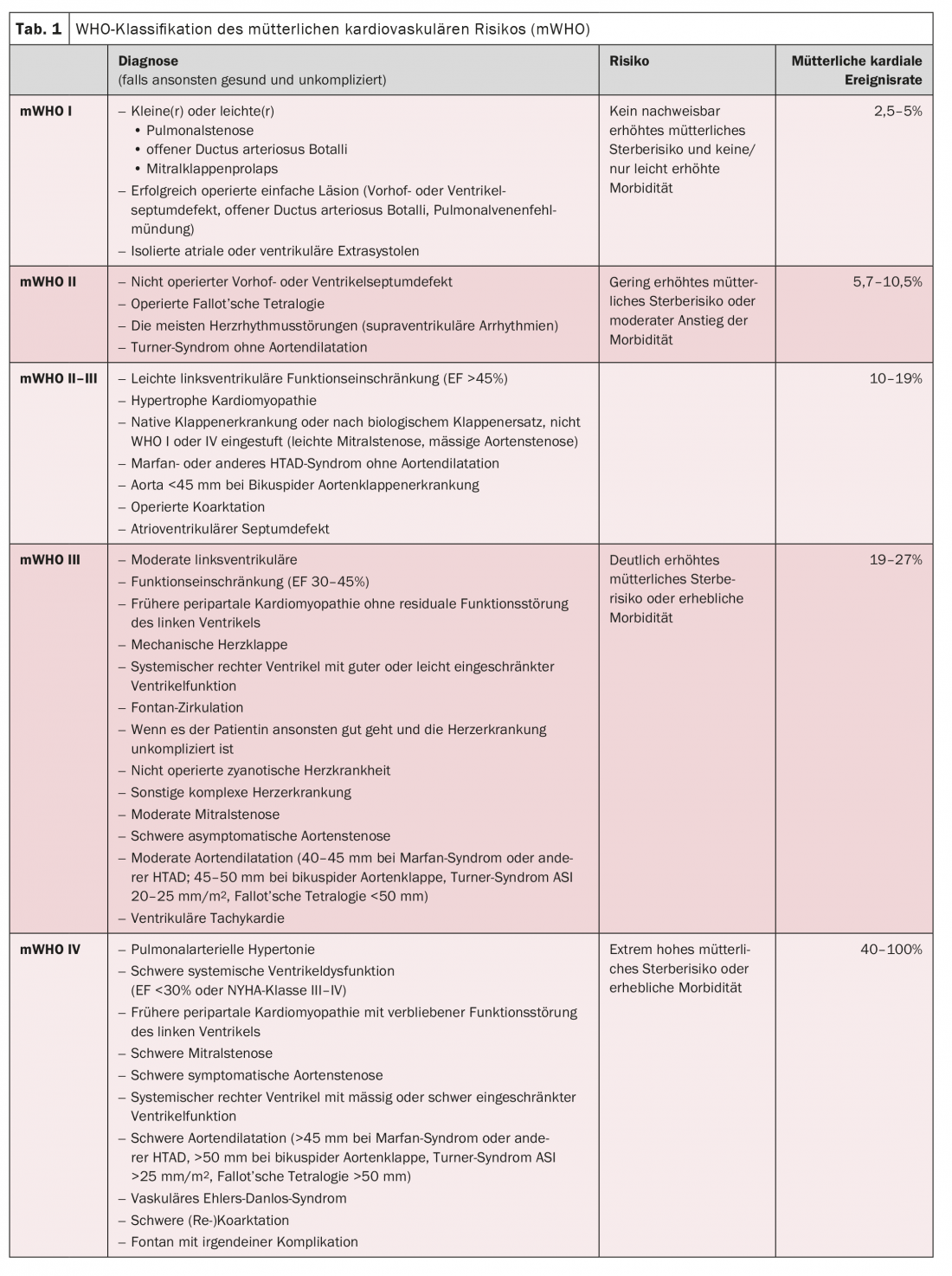
The care of patients at increased cardiovascular risk during pregnancy is becoming increasingly common. Then an interdisciplinary treatment concept involving gynecology, cardiology, pediatric cardiology, neonatology, cardiac surgery, anesthesiology and cardio-anesthesiology is required. As a rule, vaginal delivery is recommended unless premature induction of labor is indicated or the patient meets WHO maternal cardiovascular risk (mWHO) classification IV (Table 1) . In this way, the mortality of mother and child can be significantly reduced. However, care should be taken to ensure that disciplines are closely networked and maintain good communication. This is because the care of female patients with cardiovascular disease can be very complex and requires a small-scale and highly individualized approach. Fortunately, however, atrial fibrillation is a problem that occurs only sporadically in this clientele. Ventricular arrhythmias or valve diseases are much more common in practice.
Sources: Detection of atrial fibrillation with established and emerging technologies: standards 2022. and atrial fibrillation and other arrhythmias in pregnancy. 88th Annual Meeting of the DGK, Mannheim, 20-22 April 2022.
CARDIOVASC 2022; 21(2): 20-21









