Vascular dementia (VaD) is the second most common cause of dementia after Alzheimer’s dementia and thus the most common non-neurodegenerative form of dementia. It does not represent a singular disease. Of particular clinical importance is the cerebral microangiopathy often associated with hypertension, which can lead to subcortical ischemic vascular dementia (SIVD). This is probably the best characterized form of VaD and is characterized less by memory impairment and more by executive function and processing speed impairments. The diagnosis is based in particular on anamnestic, clinical and imaging examinations. In any case, it should be done at an early stage.
In the near future, against the background of the demographic development in the western industrial nations, an increasing prevalence of dementia diseases is to be expected. Due to the resulting medical as well as socio-economic implications, the Swiss “National Dementia Strategy 2014-2017” of the Federal Office of Public Health was recently adopted [1].
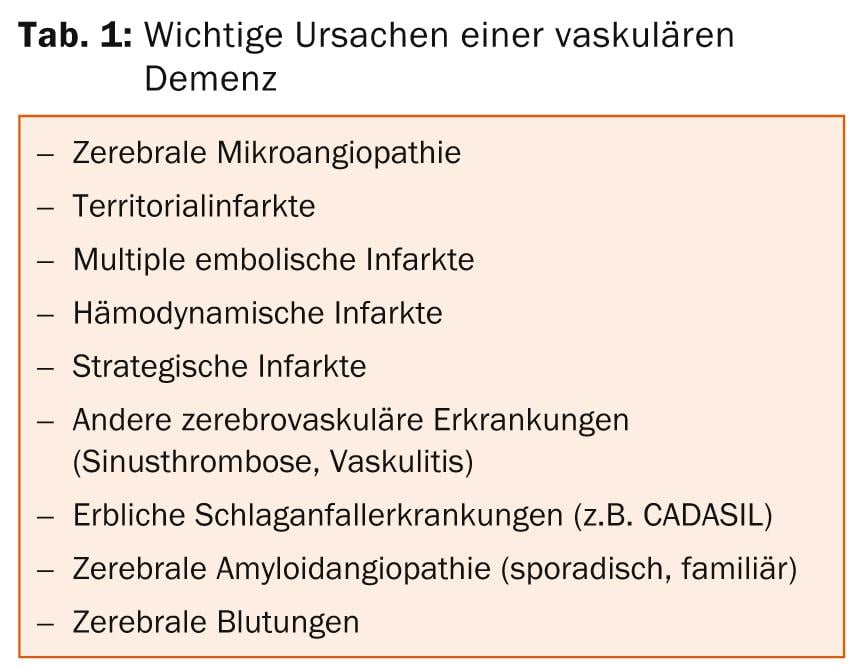
In addition to Alzheimer’s dementia (AD), which is the most common cause of dementia, vascular dementia (VaD) plays an important role as the second most common form and the most frequent cause of non-neurodegenerative forms of dementia [2,3]. Men – in contrast to AD – are affected about twice as often as women overall. Possible causes of VaD are summarized in Table 1 for reference. AD and VaD, as well as mixed forms of the two (“mixed dementia”), account for up to 80% of dementias. The latter include not infrequently occurring overlaps between AD and VaD. Vascular processes also play a significant role in the development of dementia in the context of AD [4–7], so that today both forms are also regarded as a continuum.
Classification of vascular dementia
VaD is not a single disease, but an umbrella term for a variety of cerebrovascular diseases that can lead to cognitive decline and even dementia (Table 1).
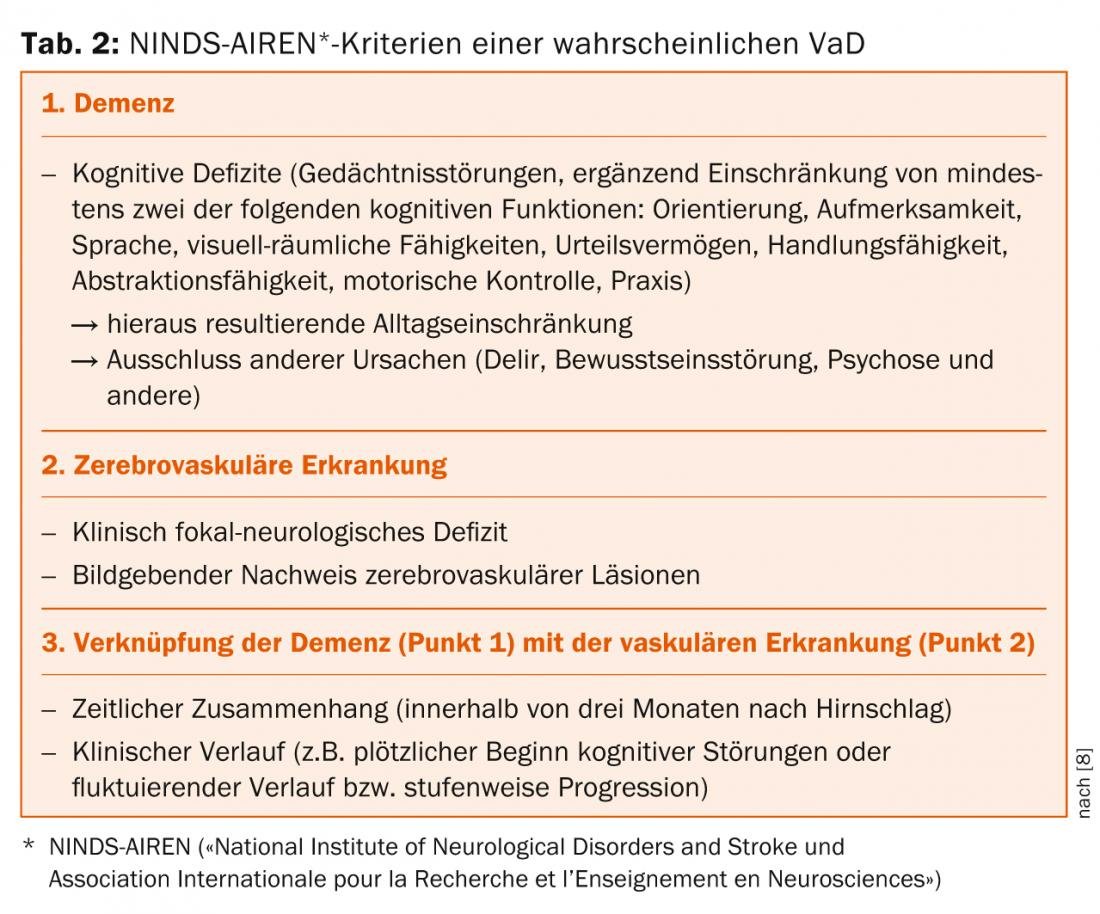
The NINDS-AIREN criteria [8], which are based on the presence of dementia and cerebrovascular disease (Table 2 ), are still used today as the valid system for diagnosing VaD. In addition, standardized criteria are used for the classification and diagnosis of vascular cognitive disorders [9].
Cerebral microangiopathy
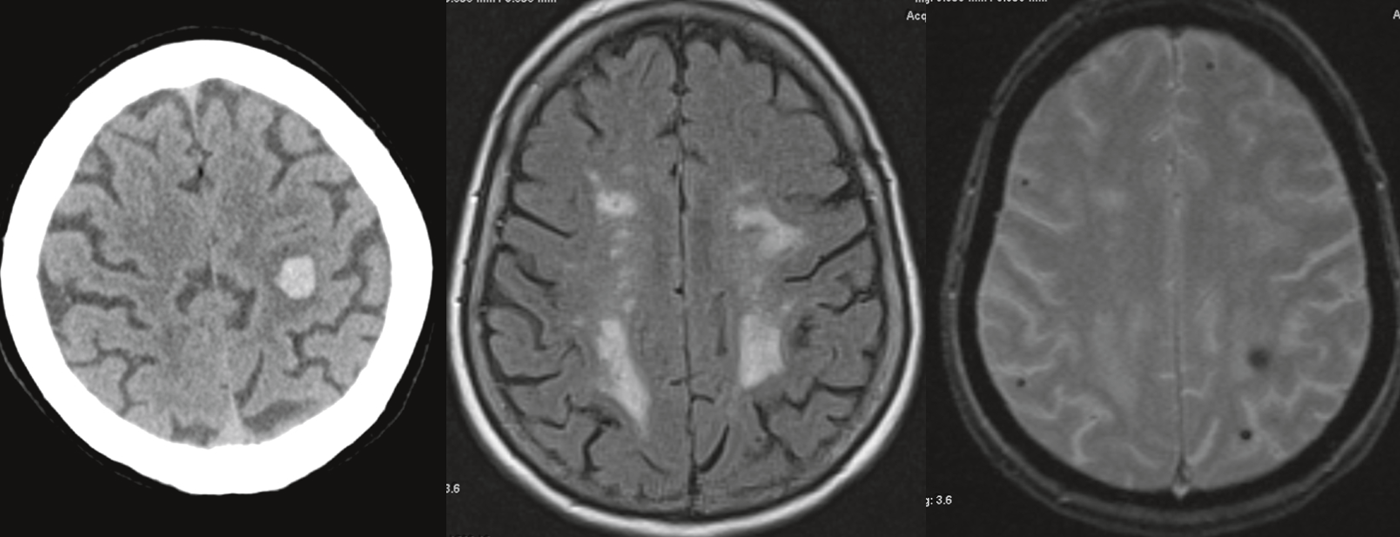
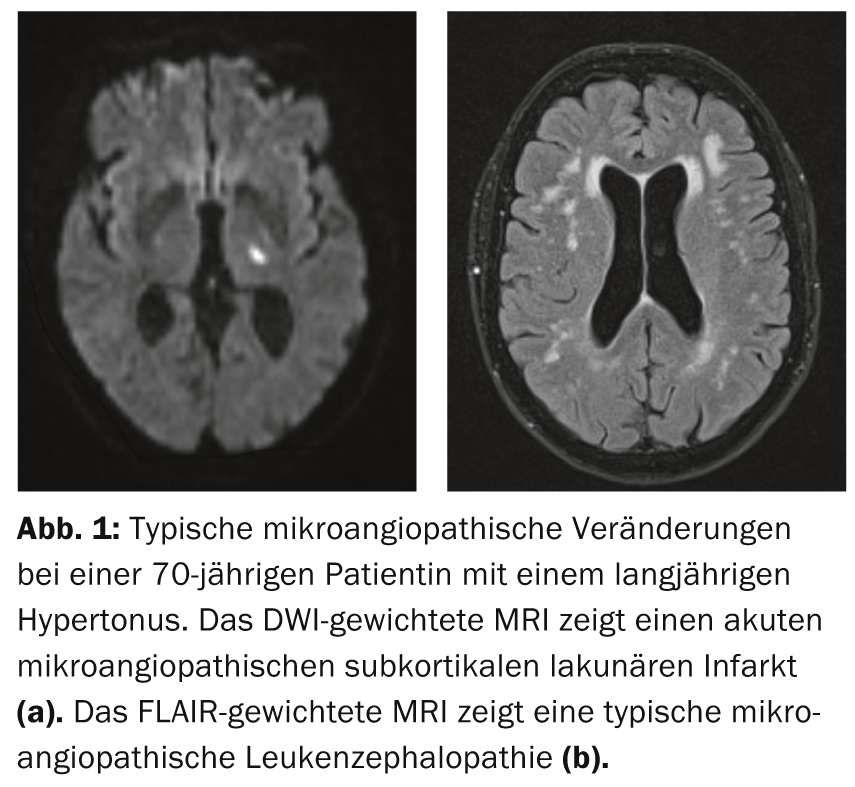
The most common cause of VaD is cerebral microangiopathy, which is particularly associated with arterial hypertension. In addition to this sporadic form, rarer hereditary forms of microangiopathy also exist, usually with a positive family history of cerebral stroke or cognitive impairment, possibly without existing vascular risk factors. About one third of all ischemic strokes are caused by cerebral microangiopathy. These lead to typical ischemic brain lesions that can be visualized by MRI imaging: Lacunar subcortical infarcts occur (Fig. 1a) as well as vascular leukencephalopathic changes in the area of the medullary canal. (Fig.1b). In addition, microhemorrhages can sometimes be found, which in microangiopathy are often localized in the area of deeper structures (e.g., basal ganglia).
In addition to physical clinical signs and symptoms (focal neurologic deficits, voiding dysfunction, gait disturbance), cognitive dysfunction is clinically prominent in microangiopathies. These not infrequently occur in a fluctuating as well as insidiously progressive manner and need not be associated with a clinically detectable stroke. Due to pathology in the area of the small arterial cerebral vessels penetrating subcortically, so-called subcortical ischemic vascular dementia (SIVD) occurs in the context of medullary ischemia. This is considered the most common form of VaD and is thus of particular importance in clinical practice. Compared to AD, it is characterized much less by memory impairment and more by executive function and processing speed impairments [10]. Thus, in its pure form, it is often clinically distinct from AD. Ultimately, microangiopathy also leads to brain atrophy, which is associated with progression of cognitive deficits [11]. In particular, arterial hypertension is a risk factor for brain atrophy due to microangiopathy. This underpins the clinical relevance of adjusting blood pressure as well as vascular risk factors overall.
Diagnostics and differential diagnostics
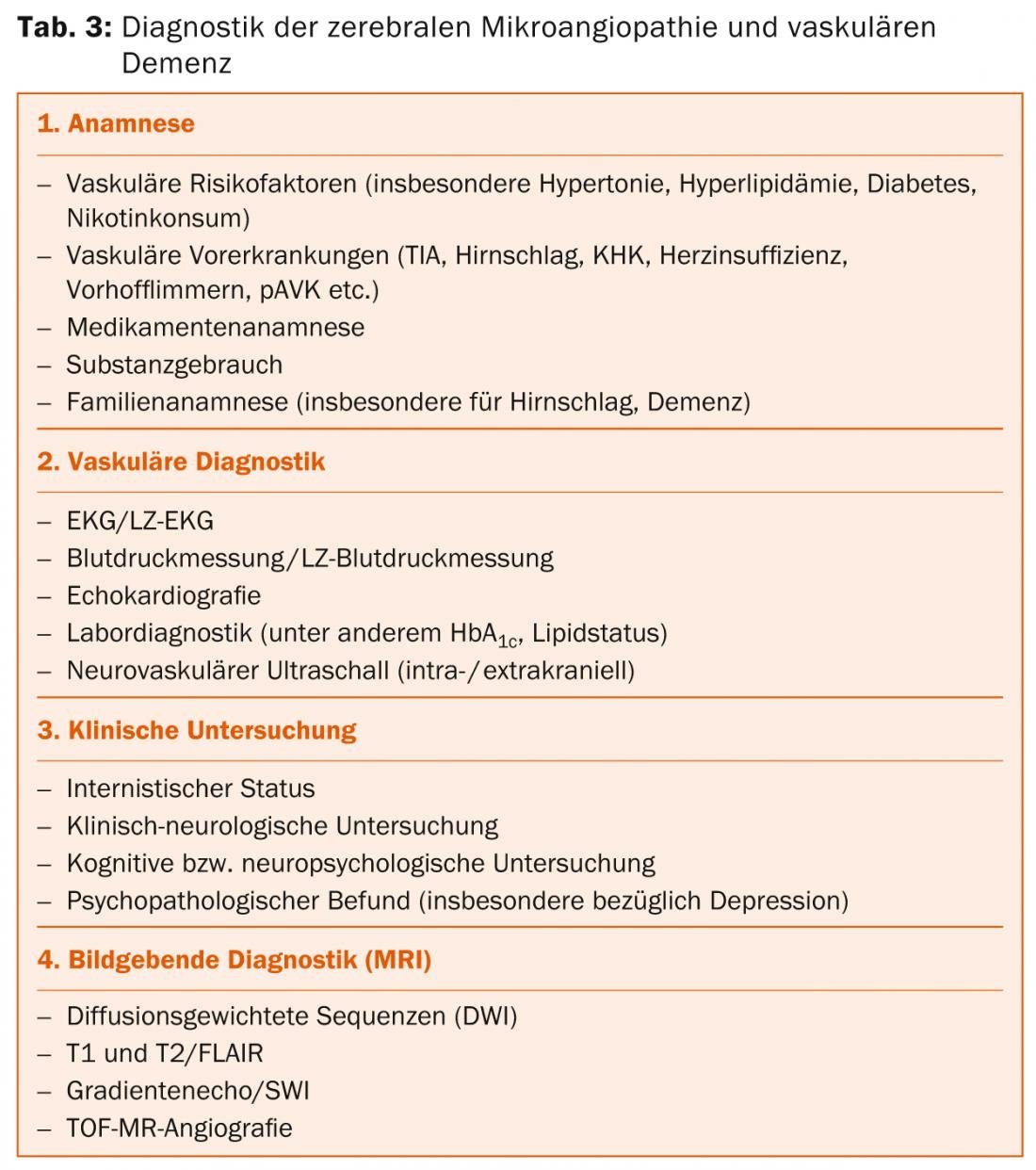
The diagnostic classification of cerebral microangiopathy and its associated VaD is based on anamnestic, clinical, and imaging parameters. An overview can be found in table 3.
An initial assessment of cognitive impairment is often already possible during the medical history interview. An external history of relatives is of great importance here, among other things with regard to possible limitations in daily life. In particular, cognitive impairments that indicate disorders of attention, concentration, and executive function disorders should be inquired about. Cognitive short test procedures are available as basic diagnostics for the first orienting assessment and quantification of cognitive impairments. These can be used well in clinical routine and can also serve as progression parameters if necessary. Here, for example, the Mini-Mental-Test, the DemTect, TFDD (test for early dementia detection with depression delineation) or the German-language version of the MoCA (“Montreal Cognitive Assessment”) should be mentioned, although these test procedures are not specifically aimed at VaD. Alternatively, for vascular cognitive impairment, two shorter (5- and 30-minute) testing procedures have been proposed for routine clinical use [9], which may better capture the aforementioned characteristic deficits in microangiopathy. The so-called trail making test is also suitable for this purpose.
Clinical neurological examination often reveals disinhibited primitive reflexes (palmomental reflex, grasping reflex, etc.) and impaired postural reflexes. In addition to ischemia-related focal neurologic deficits, extrapyramidal motor disturbances may also become apparent in advanced stages of the disease.
Diagnostic imaging by MRI (Table 3) is aimed , on the one hand, at detecting fresh (DWI) or older (T2/FLAIR) vascular lesions (Fig. 1).
In particular, the typical ischemic medullary lesions that can be detected in the T2/FLAIR evaluation should be mentioned here, which can occur in a wide variety of manifestations up to a confluent leukoencephalopathy. Such changes are a common finding with increasing age. In addition, the question of lacunar substance defects (T1) as well as hemorrhages or microhemorrhages (T2*/SWI) arises.
In addition, imaging is used to exclude other cerebral pathologies that may lead to a dementing syndrome (e.g., NPH, inflammatory lesions, tumors, regional or global atrophy in the setting of a neurodegenerative disease).
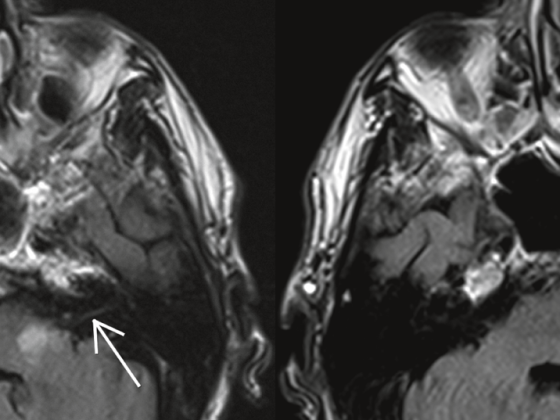
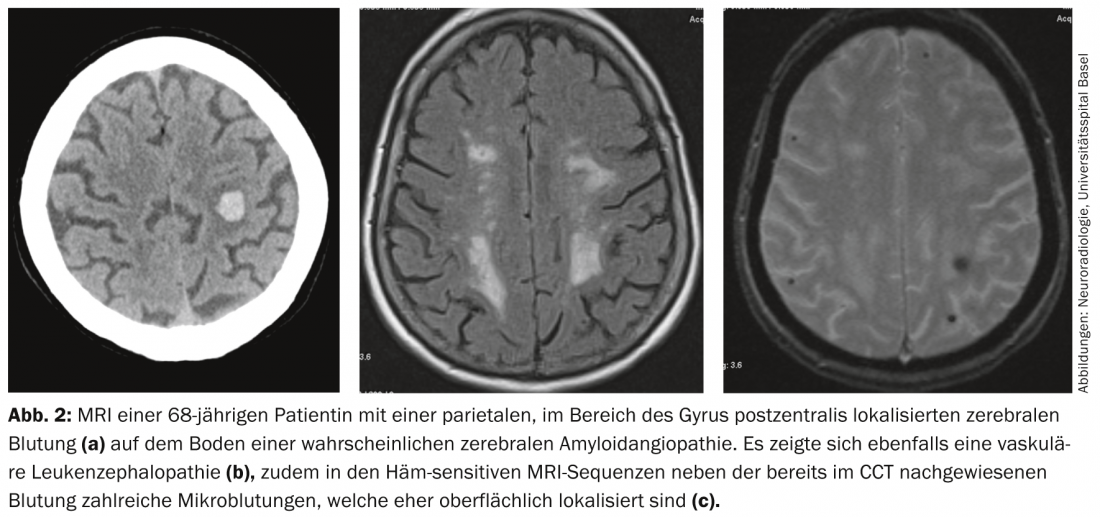
An important differential diagnosis of cerebral microangiopathy – especially in the elderly – is cerebral amyloid angiopathy (CAA) (Fig. 2), which can also lead to VaD. Differential diagnosis is particularly important because CAA is associated with cerebral hemorrhage, which has direct therapeutic implications, e.g., for the use of platelet aggregation inhibitors in a patient with vascular leukoencephalopathy.
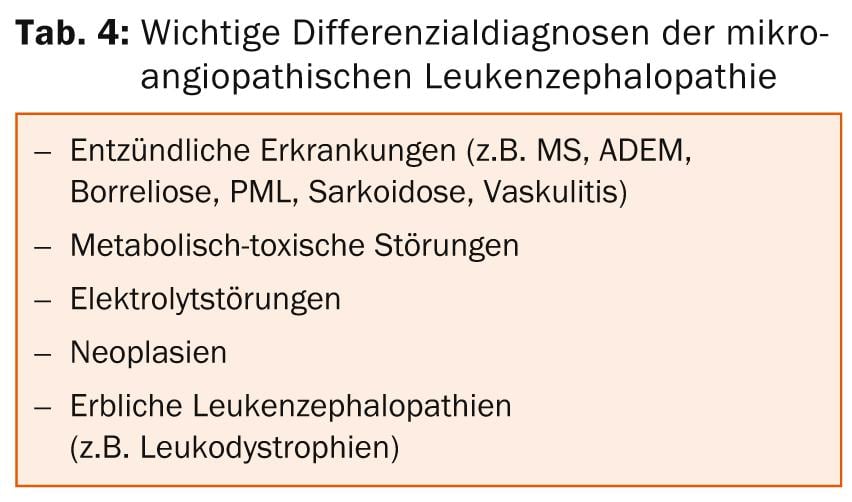
Sometimes the differential diagnosis of microangiopathic ischemic medullary lesions from other nonvascular causes of leukoencephalopathy can be challenging.
Important differential diagnoses are listed in Table 4. Inflammatory and metabolic diseases are particularly worthy of mention here. If necessary, further tests, in particular cerebrospinal fluid (CSF), laboratory chemistry, and serology, should be considered to differentiate the leukoencephalopathy from a microangiopathic vascular etiology.
Therapy
Underlying vascular diseases: Treatment in VaD is aimed particularly at early control of existing vascular disease and risk factors, and in microangiopathy, particularly at blood pressure control. In this context, blood pressure control per se is more important than the use of specific substance groups, although antihypertensives acting on the renin-angiotensin system may play a special role in this context. Because the occurrence of a clinically manifest stroke is per se a risk factor for VaD, risk factor control in terms of primary prevention of cerebrovascular disease is important. Accordingly, the same applies equally to secondary prevention of cerebral strokes, as recurrent stroke causes a further, significant increase in the risk of VaD [12]. Thus, secondary prophylaxis with drugs according to current guideline recommendations also plays an important role in the context of vascular cognitive disorders.
For the primary prophylactic use of e.g. platelet aggregation inhibitors for dementia therapy/prophylaxis, no clear data are available today, so that this is currently not recommended. This also applies to the use of statins. Counseling should be provided regarding modifiable lifestyle factors, particularly alcohol and nicotine use and physical activity. Thus, overall, the therapy of vascular factors and diseases plays an important role in dementia prevention and treatment, not least because therapeutic approaches to AD as a neurodegenerative disease have been limited to date.
Symptomatic therapy: If there is evidence for the presence of mixed dementia, symptomatic therapy as in AD is currently recommended, provided there are no vascular contraindications, e.g., against the use of cholinesterase inhibitors. In the case of concomitant neuropsychiatric symptoms, the use of atypical neuroleptics in particular should be critically reviewed in light of a potentially increased risk of cerebrovascular complications. Conventional neuroleptics should also be avoided because of potential anticholinergic and extrapyramidal motor side effects. Symptoms of depression should not be treated with anticholinergic antidepressants (such as tricyclics); selective serotonin reuptake inhibitors (SSRIs), for example, are an option here.
Summary
The term VaD does not describe a singular disease, but rather a general dementia syndrome based on cerebrovascular disease. Cerebral microangiopathy is the most common cause of VaD. It is often associated with arterial hypertension and leads to subcortical cognitive impairment in particular. Thus, the profile of cognitive disorders differs from AD, but overlap and hybrid forms are not uncommon.
Cerebral imaging has a critical diagnostic role in addition to clinical neurologic assessment. Early diagnosis of vascular causes of cognitive impairment should lead to initiation of therapeutic or preventive measures. Cerebral microangiopathy can have a significant negative impact on the course of Alzheimer’s disease. This underlines the importance of early diagnosis and therapy.
Ischemic stroke is a major risk factor for the occurrence of vascular cognitive impairment. Optimized primary preventive risk factor control as well as secondary prophylaxis are therefore of great therapeutic importance also with regard to VaD.
PD Nils Peters, MD
Literature:
- National Dementia Strategy 2014-2017, Federal Office of Public Health (FOPH) and Swiss Conference of Cantonal Ministers of Health (GDK). Bern, November 2013.
- Roman GC, Kalaria RN: Neurobiol Aging 2006; 27: 1769-1785.
- Stevens T, et al: Br J Psychiatry 2002; 180: 270-276.
- Heyman A, et al: Neurology 1998; 51: 159-162.
- O’Brien JT, et al: Vascular cognitive impairment. Lancet Neurol 2003; 2: 89-98.
- Roman GC: Neuroepidemiology 2003; 22: 161-164.
- Snowdon DA, et al: JAMA 1997; 277: 813-817.
- Roman GC, et al: Neurology 1993; 43: 250-260.
- Hachinski V, et al: Stroke 2006; 37: 2220-2241.
- Peters N, et al: Am J Psychiatry 2005; 162: 2078-2085.
- Peters N, et al: Neurology 2006; 66: 1517-1522.
- Pendlebury ST, Rothwell PM: Lancet Neurol 2009; 8: 1006-1018.
InFo NEUROLOGY & PSYCHIATRY 2014; 12(3): 18-21.