
Like many things, the acceptance of tattoos is subject to social changes and time currents. Obviously, for thousands of years, people have felt the need to use tattoos to differentiate themselves from others or to show that they belong to a socio-cultural group.
Like many things, the acceptance of tattoos is subject to social changes and time currents. Obviously, for thousands of years, people have felt the need to use tattoos to differentiate themselves from others or to show that they belong to a socio-cultural group. Examples of this are tattoos from the Bronze Age, in Egyptian mummies or in primitive peoples such as the Maori in Polynesia [1]. The discovery of the so-called glacier mummy “Ötzi” in the South Tyrolean Alps in 1991 achieved worldwide fame. The Neolithic mummy is dated to the period 3350-3100 years BC and has very numerous tattoos. The currently oldest tattooed mummies with a date of origin of about 5350 years BC can be found in the British Museum in London. A bull and a sheep or goat could be identified on a male mummy using CT and infrared technology on the right upper arm as the Süddeutsche Zeitung reported in an article on March 5, 2018. In our latitudes, tattoos were considered until well into the second half of the 20th century rather stigmas of little respected social groups such as criminals, traveling people prostitutes and sailors. Still at the beginning of the 20th century, heavily tattooed people and especially women were displayed as attractions at fairs, in show booths and in the circus to serve the needs of bourgeois society for exoticism and eroticism [2].
Today, tattoos are considered beautiful, stylish and an expression of individual lifestyle in broad sections of society. Acting stars, sports idols and the new social networks are still reinforcing trends, and certain tattoo artists already enjoy cult and artist status among tattoo followers. The industry is booming. Scientifically really exact numbers are not to be elicited, but according to estimations in Great Britain every third person between 16 and 44 years is tattooed [3]. In Germany alone, 8 million people are said to wear tattoos, which would correspond to about 10% of the total population. The figures for Switzerland are likely to be similar in proportion.
At the 2017 SGML Congress, Dr. Heike Heise of Germany reported that 39% more tattoos were removed in 2015 than in 2014. Many would also like to have the “youth sins” removed again [4]. Annual increases of 20% could realistically be expected. It is estimated that 16-44% regret at least one of their tattoos and 21-50% of you are looking into tattoo removal or partial removal [5,6,18]. So the potential market for tattoo removal is large. Industry and the medical profession, and unfortunately also questionable providers, have long since discovered this development for themselves.
Fortunately, since June 1, 2019, the legislature in Switzerland has placed a very high priority on patient protection with the Federal Act on Protection against Hazards from Non-Ionizing Radiation and Sound (NISSG) and put an end to the dangerous “proliferation” of insufficiently qualified providers. The associated ordinance now clearly states which treatments are subject to a doctor’s reservation, i.e. may only be performed by a doctor or directly instructed practice staff. Directly instructed practice personnel are persons employed by a physician and working under the physician’s direct control, supervision and responsibility. Third parties who, for example, rent premises in a medical practice but carry out their activities independently are not covered by this. Until June 1, 2024, there are still transitional periods for persons who do not meet these criteria, during which they can acquire the certificate of competence “Competent person for NIR and sound for cosmetic purposes”. Without this certificate of competence, the aforementioned group of persons may no longer treat tattoos with lasers after June 1, 2024.
Laser therapy for tattoo removal
Goal: In most cases, the goal of laser therapy is the most gentle, complete, scar-free removal or partial removal of the offending tattoo. Recently, however, we have also had an increase in requests that only want the tattoo to be lightened for a “cover-up” (overstitching).
Methods: Laser is the gold standard for tattoo removal. Destructive procedures such as dermabrasion, application of acids, cryosurgery, excisions or ablation withCO2 lasers are actually to be rejected today because of their often considerable side effects such as hypopigmentation and scarring and also no longer meet our aesthetic as well as ethical requirements [7].
Laser therapy is based on the “principle of selective photothermolysis” formulated by Anderson and Parrish in 1983, which states that, if possible, only the target structure should be hit while sparing the surrounding tissue as much as possible [8]. Specifically, this means:
- The wavelength must correspond to the target chromophore.
- The pulse length must be shorter than the thermal relaxation time of the respective target structure so that selective thermolysis is possible and the surrounding structures are little affected.
- The energy depends on the target structure and must be sufficiently high in the short pulse time to really destroy the target structure.
Since lasers can only produce coherent light (light of one wavelength), it is still not possible to remove all colors perfectly with a laser. Up to now, Q-switched laser systems have been used, which must be based on the wavelength of the pigments to be treated [9]:
- qs-KTP-Nd.: YAG laser (532 nm) for red , orange, brown
- qs ruby laser (694 nm) for black, blue, green, brown
- qs alexandrite laser (755 nm) for black, blue, green, brown
- qs-Nd:YAG laser (1064 nm) for black blue
Certain colors such as orange, yellow and violet are still often difficult and unsatisfactory to remove. The color white cannot be removed because there is no target chromophore for the laser.
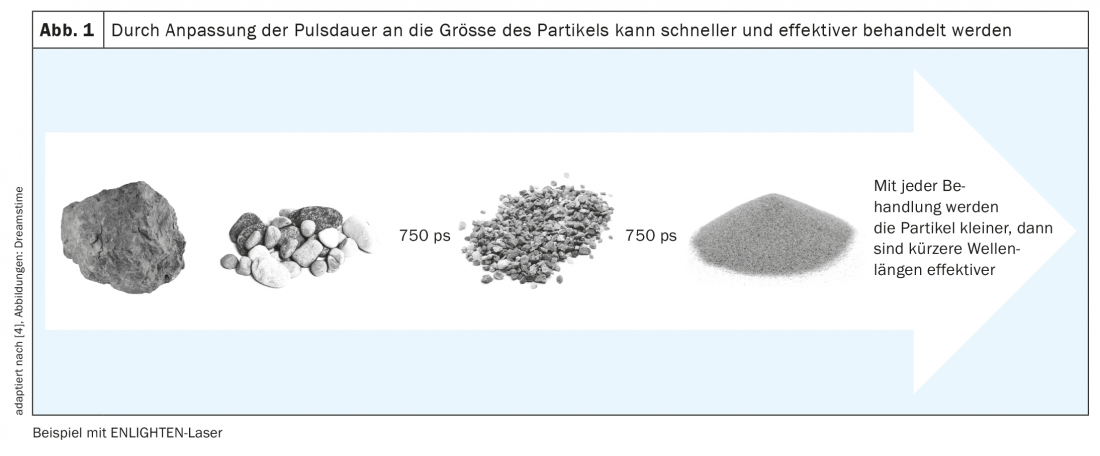
The basic principle is to break up the introduced pigments very strongly by the laser energy so that they are no longer visible to the human eye (Fig. 1).
The inflammatory reaction leads to the activation of macrophages, which take up pigments via phagocytosis and subsequently transport them away via the lymphatic system. The idea that patients often have of simply erasing a tattoo is unfortunately not realistic.
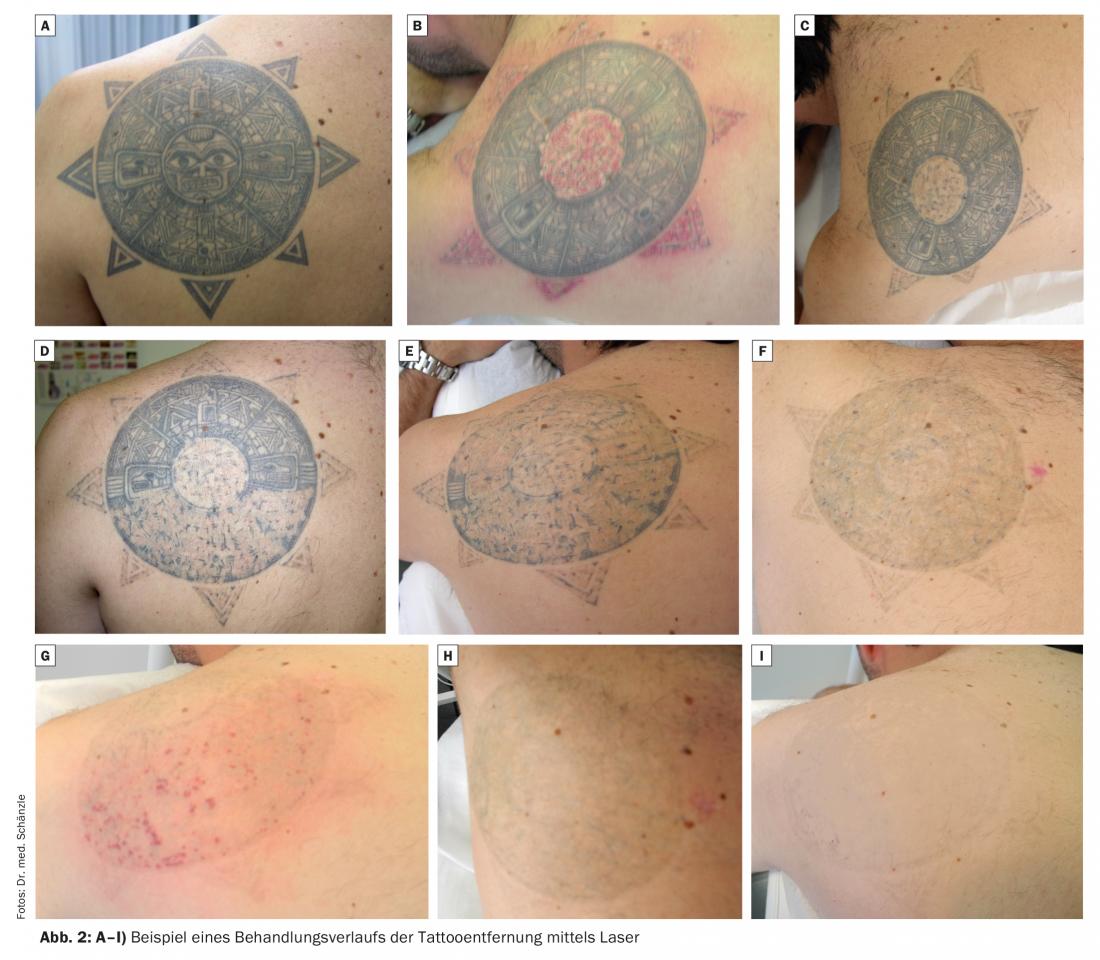
In principle, we distinguish between amateur and professional tattoos, whereby the former are usually much easier and can be removed with fewer treatment sessions. For professional tattoos, we usually assume 8-12 treatments in our clinics, although significant variations can occur (Fig. 2 A-I) [10].
In recent years, a new addition is the use of picosecond lasers, which most likely have relevant advantages in tattoo removals in terms of number of sessions, painfulness and removal of difficult colors. Ultra-short pulse times and the choice of different wavelengths (e.g., 532 nm, 595 nm, 660 nm, 775 nm, 1064 nm) should enable even greater decomposition of the target structures. However, the acquisition costs are still very high and a final assessment is not yet given [11,12].
Further optimization possibilities could be a repeat treatment after 20 minutes with Q-switched lasers [13] and the combination with fractional lasers [14].
Several complementary treatment protocols to the above treatment options have been published [15,16].
Practical procedure
How many sessions are really required can never be accurately predicted, as we never know exactly how dense, how deep the stitching is, and exactly what the introduced pigments are composed of. It is essential to explain this to the patient in detail during the preliminary discussion. In the case of permanent make-up, we always recommend a trial laser treatment of a small area first, in order to be able to better assess the color changes (ink darkening) that occur frequently and are sometimes problematic. The treatment intervals should not be too short. We prefer intervals of 2 months and initially treat with low energy densities [17].

If the wavelength, energy density and pulse length are set correctly, a slight acoustic popping sound should be emitted, as well as whitening, which is caused by local heating of the pigment with plasma and gas formation and subsequent dermal and epidermal vacuolization. (Fig. 3). Small spot hemorrhages and posttherapeutic urticarial skin reactions occur frequently and are not problematic (Fig. 4). As a rule, we do not perform any local anesthetic measures beforehand, but the use of powerful cold air devices shortly before, during and after the treatment has proven very effective for us. We often treat large tattoos fractionally to avoid too much pain and complications such as lymphedema.

After these general remarks, I would now like to present our counseling and education concept specific to the Pallas Clinics and Pallas Centers, which, in addition to effective treatment, plays a central role for us in the success of treatment and patient satisfaction:
- The initial consultation is conducted by a dermatologist experienced in laser therapy.
- He first discusses the patient’s expectations (removal, partial removal, whitening)
- This is followed by clinical inspection and assessment of the tattoo (single color, multi-color, micro-scarring, size, easy or difficult to remove colors, amateur or professional tattoo, etc.).
- Obligatory going through the checklist (overview 1) before tattoo laser
- Detailed information about potential NW (pigment shift in the form of hypo- and hyperpigmentation, scarring, blistering, infection, etc.).
- Estimating the frequency of treatment sessions and providing a prognosis on the expected success of treatment, setting the treatment price per session.
- Photo documentation, informed consent and treatment contract
- Arrangement 1st treatment appointment.
Literature:
- Schönewolf N, et al: Tattoos and how to get rid of them. Switzerland Med Forum 2010; 10(19-20): 340-343.
- Eberhard I: The queen of the tattooed and other tattooed ladies – tattooed showmen in show booth and circus. Practical Dermatology 2017; 536-554.
- Hardning E: More than a quarter of middle-class people admit to having a tattoo with letters and scripts proving most popular. Daily Mail, 2014. www.dailymail.co.uk/news/article-2714837 (as of August 3, 2014).
- Ramm-Fischer A: Modern tattoo removal. Dermatology and Aesthetic Medicine 2017 (2): 18-20.
- Kurniadi I, et al: Laser tattoo removal: Fundamental principles and practical approach. Dermatol Ther 2021; 34(1): e14 418.
- Liszewski W et al: The Demographics an Rates of Tattoo Complications, Regret, and Unsafe Tattooing Practices: A Cross-Sectional Study. Dermatolg Surg 2015; 41(11): 1283-1289.
- Hammes S, Raulin C: Removal of tattoos – State of the art 2017. Practical Dermatology 2017(6): 523-535.
- Anderson RR, Parrish JA: Selective photothermolysis: precise microsurgery by selection absorption of pulsed radiation. Science 1983; 220: 524-527.
- Pfirrmann Karsai S, et al: Tattoo removal-state of the art. J Dtsch Dermatol Ges 2007; 5(10): 889-897.
- Bencini PL, et al: Removal of tattoos by q-switched laser: variables including outcome and sequelae in a large cohort of treated patients. Arch Dermatol 2012; 148(12): 1364-1369.
- Karsai, Bäumler W, Raulin C: Laser tattoo removal: is there light at the end of the tunnel or is it just the light of an oncoming train? Br J Dermatol 2016; 175(6): 1338-1339.
- Baumler W, et al: The efficacy and the adverse reactions of laser assisted tattoo removal-a prospective split study using nanosecond an picosecond lasers. J Eur Acad Dermatol Venereol 2022; 36(2): 305-312.
- Kossida T, et al: Optimal tatoo removal in a single laser session based on the method of repeated exposures. J Am Acad Dermatol 2012; 66(2): 271-277.
- Radmanesh M, Rafiei Z: Combination of CO2 an Q-switched Nd: YAG lasers is more effective than Q-switched Nd: YAG laser alone for eyebrow tattoo removal. J Cosmet Laser Ther 2015; 17(2): 65-68.
- Weiss ET, et.al: Combining fractional resurfacing and Q-switched ruby laser fpr tatto removal. Dermatol Surg 2011; 37(1): 97-99.
- Narayanan A: A split-tattoo randomized Q-switched neodymium-doped yttrium-aluminum-garnet laser trial comparing the efficacy of a novel three-pass, one-session method with a conventional method inthe treatment of blue/black tattoos in darker skin types. Clin Exp Dermatol 2022; 47(1): 125-128.
- Humphries A, et al: Finite element analysis of thermal and acoustic processes during laser tatto removal. Lasers Surg Med 2013; 45(2): 108-115.
- Heidemeyer K, Adatto M: What is new in laser tattoo removal. Dermatologica Helvetica 2022(3): 27-29.
DERMATOLOGIE PRAXIS 2022; 32(5): 14-17









