Since dizziness can have many underlying causes, diagnosis is often difficult. How can vertigo symptoms be classified? And what therapeutic measures are recommended?
For most patients with symptoms of vertigo, the primary care physician is the first point of contact. Thus, primary care physicians take on the important task of differentiating into serious and harmless forms of vertigo. Prof. Dr. med. Karl-Friedrich Hamann from Munich presented a simple diagnostic scheme at this year’s congress of the German Society for Internal Medicine.
Vestibular vertigo – a disorder of the vestibular system.
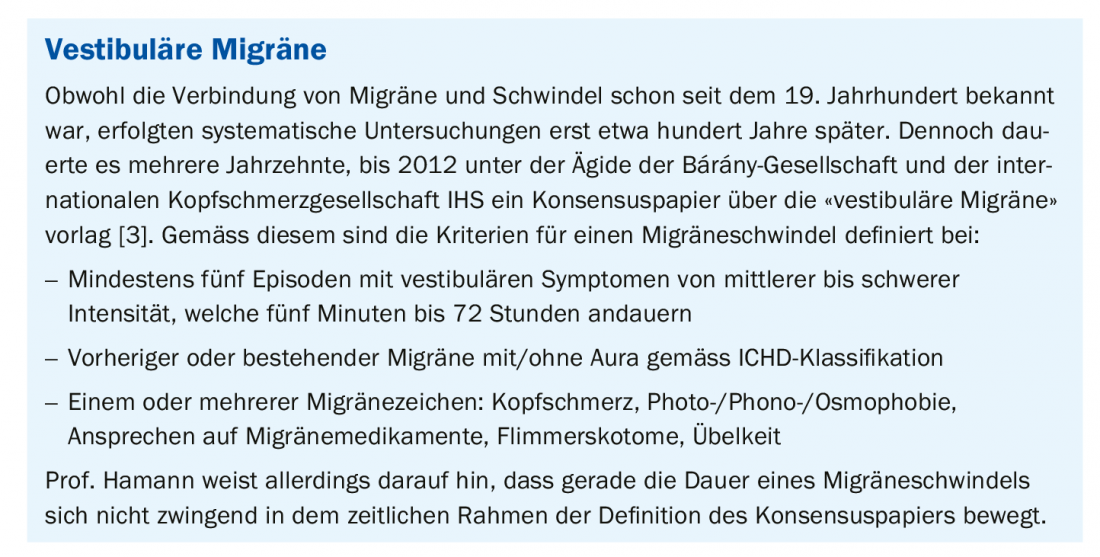
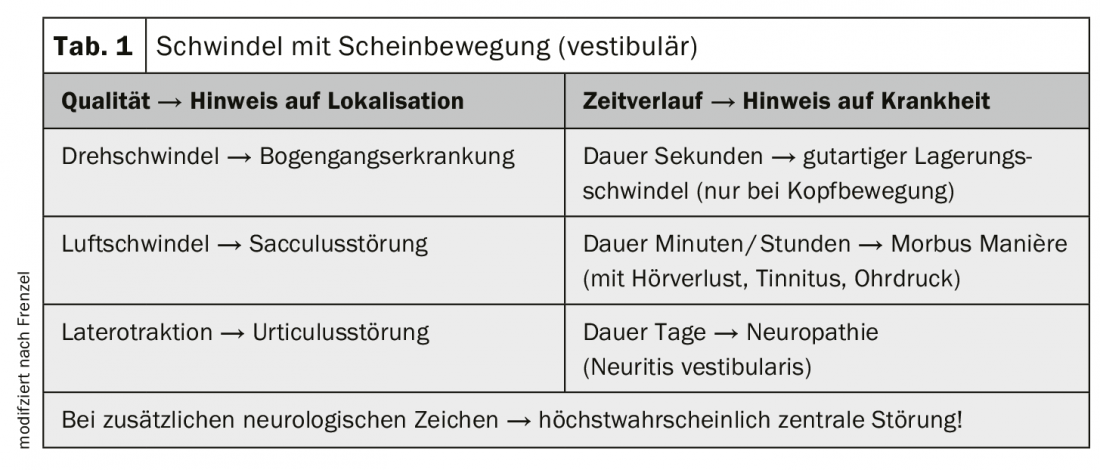
The classification of vertigo is initially based on whether or not the symptomatology is due to a vestibular disorder. In case of vertigo with apparent movements, there is most likely a disturbance in the vestibular system, since this system is responsible for motion detection. In a study that included about 1151 patients of an outpatient dizziness clinic, the most common vestibular pathologies were neuropathy (34.2%), Manière’s disease (32%), and benign positional vertigo (22%). Due to better definability (box), migraine vertigo (7%) has also statistically increased [1]. On the question of whether peripheral or central, the speaker recommends a simple rule: “The more peripheral the cause, the more severe the dizziness.” If, on the other hand, the disorder is central, dizziness is never the only symptom. Table 1 provides a simplified scheme of symptoms and possible diagnoses. Vestibular disorders can be differentiated by quality and time course. If there are also neurological signs (e.g., blurred vision, double vision, dysphagia, and speech problems), it is most likely a central disorder.
Vestibular disorders can be objectified with Frenzel’s magnifying glasses. In the darkened room, this aid enables detection of nystagmus through fixation suppression. Vibratory stimulation gives evidence of a pathological side difference; in the case of a peripheral side difference, the vibratory nystagmus always strikes out to the side of better excitability. This objectification method replaces thermal testing in many cases.
Recognize non-vestibular vertigo
If the patient complains of dizziness without apparent movements, it becomes somewhat more difficult to diagnose. This is because in these cases the cause is not a disturbed equilibrium system (Fig. 1).
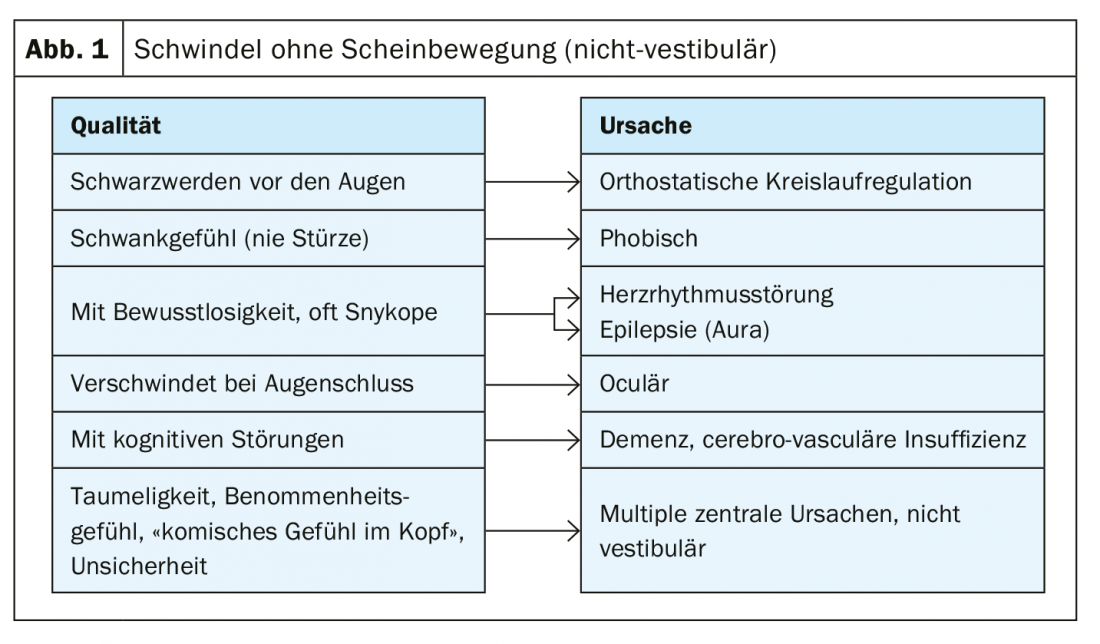
According to Prof. Hamann, the “problem child” is phobic vertigo, from which about 3% of vertigo patients suffer according to the Schwindelambulanz survey [1]. In phobic vertigo, all vestibular systems function normally. Rather, the vertigo sensation is produced by patients drawing on a past vertigo experience and reproducing it due to a processing disorder. Thus, anxiety vertigo (psychogenic vertigo) is not a directed vertigo but an undetermined vertigo, which is also called phobic vertigo. It is often situational, does not lead to falls, and has no organic correlate.
Ophthalmic vertigo disappears with eye closure. Causes can be not or incorrectly fitted glasses or varifocals.
Cardiovascular dizziness, which is an expression of a circulatory regulation disorder or a cardiac arrhythmia, is not an actual dizziness. In both bradycardic and tachycardic underlying diseases, the vertigo symptoms that occur are often very different; they range from staggering vertigo to lightheadedness to blackness before the eyes, although the severity of the underlying disease does not necessarily correlate with the severity of the vertigo. In bradycardic arrhythmias, patients sometimes feel a “bumpy” heartbeat, while tachycardic disorders can evoke a feeling of dizziness with an experienced “racing heart.” Common to all forms of vertigo, despite their diversity, is that they are often accompanied by visual disturbances or can lead to syncope. An indication of dizziness due to obstructive heart disease is when the dizziness symptoms occur primarily during physical exertion [2].
Source: DGIM 2019, Wiesbaden (D)
Literature:
- Hamann K-F, Ritscher B: Diagnostic spectrum of a supraregional neurootological outpatient clinic for vertigo, 2007.
- German Society of General and Family Medicine (DEGAM), ed: Acute dizziness in family practice. S3 guideline, April 2018. www.awmf.org/leitlinien/detail/ll/053-018.html, last accessed June 20, 2019.
- Lempert T, et al: Vestibular migraine: diagnostic criteria. J Vestib Res 2012; 22(4): 167-172.
HAUSARZT PRAXIS 2019; 14(7): 19-20