
Preterm labor is an indication of impending preterm birth. Various measures are possible to prevent premature birth, including tocolysis. In practice, it is useful to identify risk factors for preterm birth as early as possible and to counteract them if possible. This includes the treatment of infectious diseases and good adjustment of diseases of the pregnant woman (hypertension, diabetes, etc.).
Clinical assessment of preterm labor remains difficult. We rely on the following criteria – knowing that sensitivity and specificity are not proven:
- Regular contractions,
- Painful contractions,
- ≥ four contractions per 20 minutes.
The clear evidence of labor is the progress of the birth. However, this evidence usually cannot be waited for, because if you wait for cervix-opening labor, you may miss the timely start of therapy for labor inhibition. Threatened preterm birth between the 20th and the end of the 36th week of pregnancy is defined as follows:
- ≥Four contractions per 20 minutes and sonographic cervical length <20 mm.
- ≥Four contractions per 20 minutes and sonographic cervical length between 20 and 29 mm, but with positive fibronectin test.
Primary prevention
It is important to identify increased risk for preterm birth as early as possible. The risk of preterm labor is influenced by various factors (Tab. 1). One of them is the interval after a birth until the next conception: this should be at least 18 months, less than six months is unfavorable. The ideal maternal age is between 20 and 35 years. When using artificial reproductive technology (ART), multiples should be avoided whenever possible. Other preventive measures include a normal BMI, stopping smoking, “treating” poverty (nutrition, hygiene, etc.), treating sexually transmitted diseases before pregnancy, and abstaining from illegal drugs such as cocaine.
Supplementation of 800 mg/d docosahexaenoic acid (DHA) reduced preterm birth in non-risk women in several randomized trials. Administration of magnesium per os also showed indirect beneficial effects. Data on probiotics are still insufficient. Vaginal application of progesterone appears to reduce infant morbidity and also mortality. Currently, progesterone is used for two indications of singleton pregnancy: status post preterm delivery and cervical shortening (measured sonographically) in the current pregnancy.
Secondary prevention
For secondary prevention, smoking cessation is recommended. In addition, the pregnant woman should not perform physically rigorous work (night shift). Physical rest to some extent is useful, but the disadvantages of strict bed rest such as thrombosis, demineralization, cardiovascular deconditioning, constipation, gastric distention, and worsened glucose tolerance are also known. Visits at home by a midwife primarily provide emotional support. Weekly vaginal examinations have not shown a preterm birth-reducing effect. Infections of the urogenital organs should be treated with antibiotics resp. fungicides are treated. Therapy of urinary tract infections, asymptomatic bacteriuria (>100,000 germs/ml), bacterial vaginosis, Candida colpitis, and Streptococcus B colonization causes a reduction in preterm birth; for ureaplasma, the data are controversial.
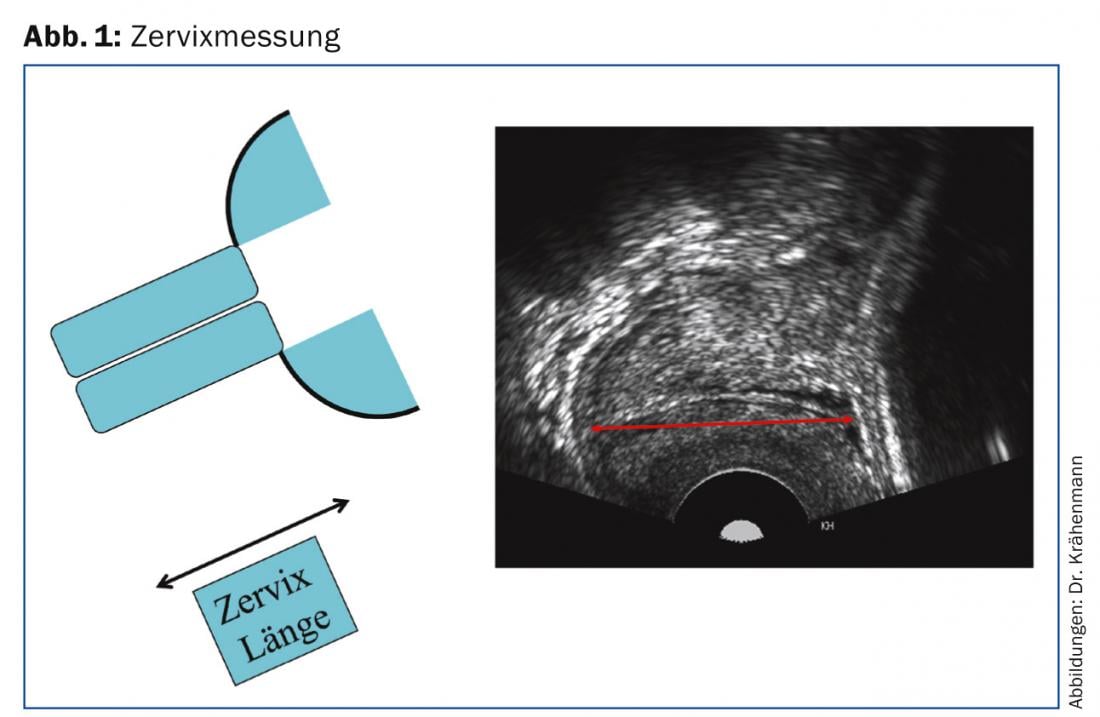
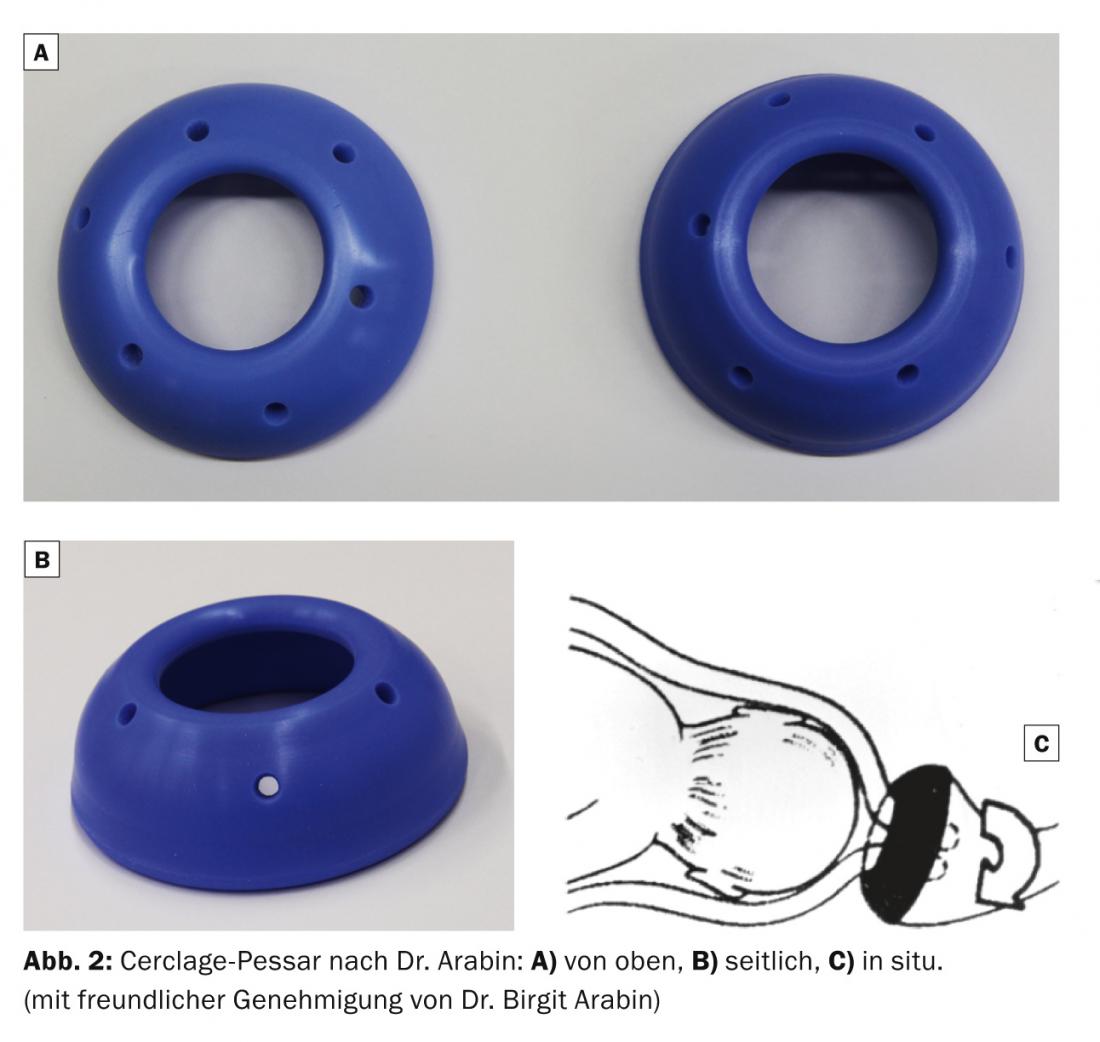
Sonographic cervical measurement (Fig. 1) with the corresponding intervention options is becoming increasingly important: Progesterone therapy and insertion of a pregnancy pessary (Fig. 2). The application of a pessary is simple and shows a favorable effect in singleton pregnancies. Presumably, the pessary acts by sacral alignment of the cervix and by preventing further funneling (V-shaped shortening of the cervix) by forming edema. The edema also forms a barrier to infection. However, contractions are an exclusion criterion for the application of a foreign body: labor must therefore be slowed down before inserting a pessary.
Measures in case of threatened premature birth
- If there is a threat of preterm birth (preterm labor or rupture of membranes), the following three questions should be answered:
- Is there an indication for acute tocolysis (up to 33 weeks gestation + 6/7 days)?
- Is there an indication for the administration of corticosteroids for fetal lung maturation (up to 33 weeks gestation + 6/7 days)?
- Should the pregnant woman be transferred to a perinatal center?
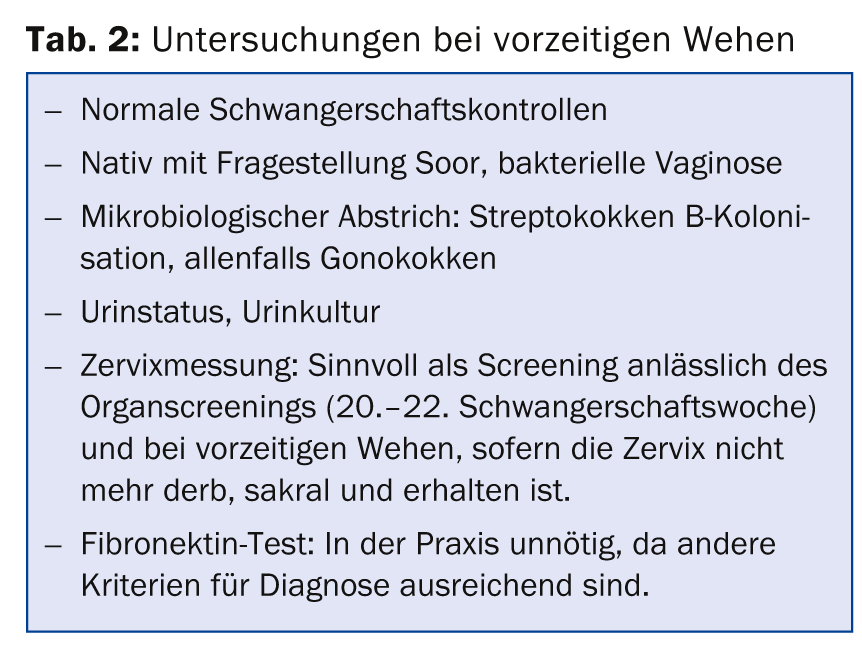
An overview of which investigations are useful in preterm labor is shown in table 2 . Possible interventions are the administration of low-dose aspirin in case of appropriate risk (e.g. status after preeclampsia), docosahexaenoic acid and/or vaginal progesterone in case of status after preterm birth or shortened cervix in the current pregnancy. In the case of a shortened cervix, the insertion of a cerclage pessary or a cerclage should also be evaluated, if necessary.
Several classes of agents are used for labor inhibition: Beta-adrenergic receptor agonists, oxytoxcin antagonists, calcium blockers, nitric oxide donors, prostaglandin synthetase inhibitors, magnesium sulfate, and herbal remedies such as Bryophyllum pinnatum. Because a calcium blocker such as nifedipine can be administered by os, this labor inhibitor is also used in practice. To date, there is no clear evidence for long-term tocolysis, but in practice, individual situations arise in which the advantages of long-term tocolysis may outweigh the disadvantages.
Franziska Krähenmann, MD, FMH, IBCLC
Marcella Siegrist-Läuchli, MD, FMH
Further reading
- “Tocolysis in preterm labor,” Swiss Society of Gynecology and Obstetrics Expert Letter 41, 2013.
http://sggg.ch/files/fckupload/file/2_Fachpersonen/Expertenbriefe/deutsch/41_Expertenbrief_2013.pdf.
CONCLUSION FOR PRACTICE
- Preterm labor is present with regular contractions, painful contractions, and ≥four contractions per 20 minutes.
- If prematurity is imminent, it must be clarified whether there are indications for tocolysis or tomodialysis. fetal lung maturation is present and whether the pregnant woman should be transferred to a perinatal center.
- In practice, it is important to identify and treat risk factors for preterm birth as early as possible.
A RETENIR
- Les contractions précoces se manifestent par un travail régulier, des contractions douloureuses et ≥ quatre cycles de contractions en 20 minutes.
- En cas de menace d’accouchement prématuré il convient d’établir si les indications pour une tocolyse, en l’occurrence une maturité pulmonaire fœtale, sont réunies et si la femme enceinte doit être transportée dans une unité de périnatologie.
- Dans la pratique, il est important d’identifier le plus tôt possible les facteurs de risque d’accouchement prématuré et de les traiter.
HAUSARZT PRAXIS 2014; 9(11): 16-18









