Lynch syndrome – often referred to synonymously as hereditary non-polyposis colon cancer – is the most common cause of hereditary colon cancer and other tumor diseases. So far, so good. But how did the disease get its name? A Search for Traces….
Lynch syndrome is an autosomal-dominant inherited tumor syndrome associated with a significantly increased risk of various cancers. This is because the patient has genetic alterations in the DNA repair genes MLH1 on chromosome 3p21.3, MSH2 on chromosome 2p21p22, MSH6 on chromosome 2p16, and PMS2 on chromosome 7p22. Unlike Hereditary Non-Polyposis Colon Carcinoma (HNPCC) – which is often used synonymously in clinical practice – the tumors do not occur exclusively in the gastrointestinal tract. There is also an increased risk of carcinoma of the stomach, endometrium, urothelial tissue, hepatobiliary system, ovaries, CNS, and skin. Because Lynch syndrome has a truncated adenoma-carcinoma sequence, even small adenomas have the potential to degenerate.
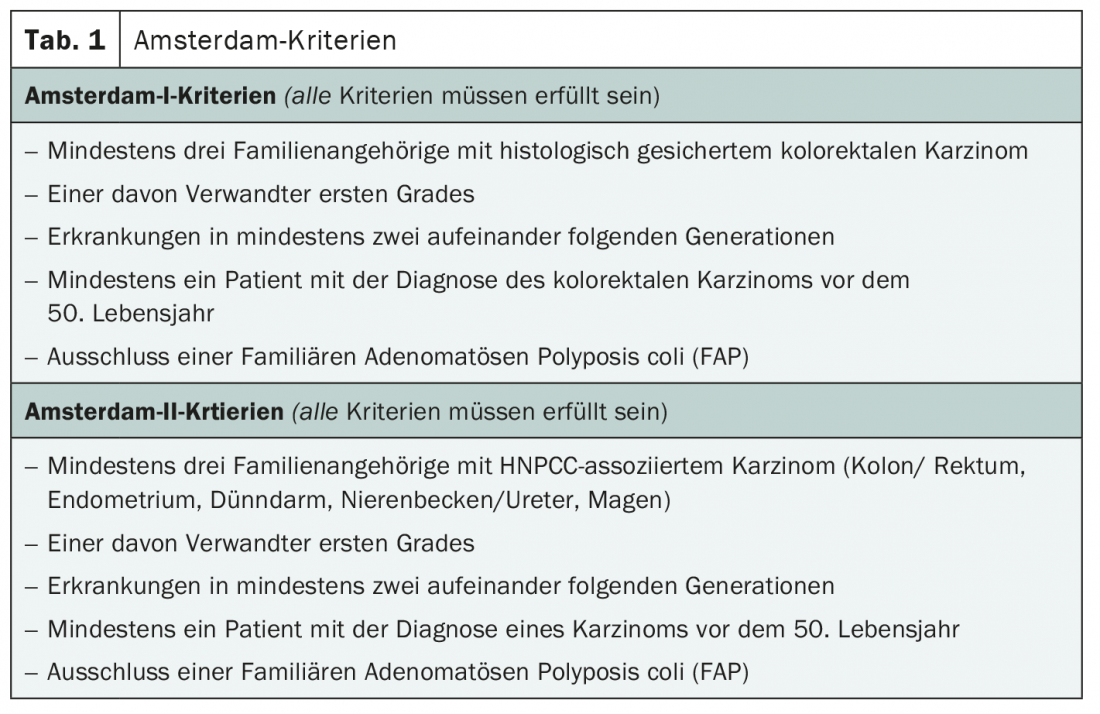
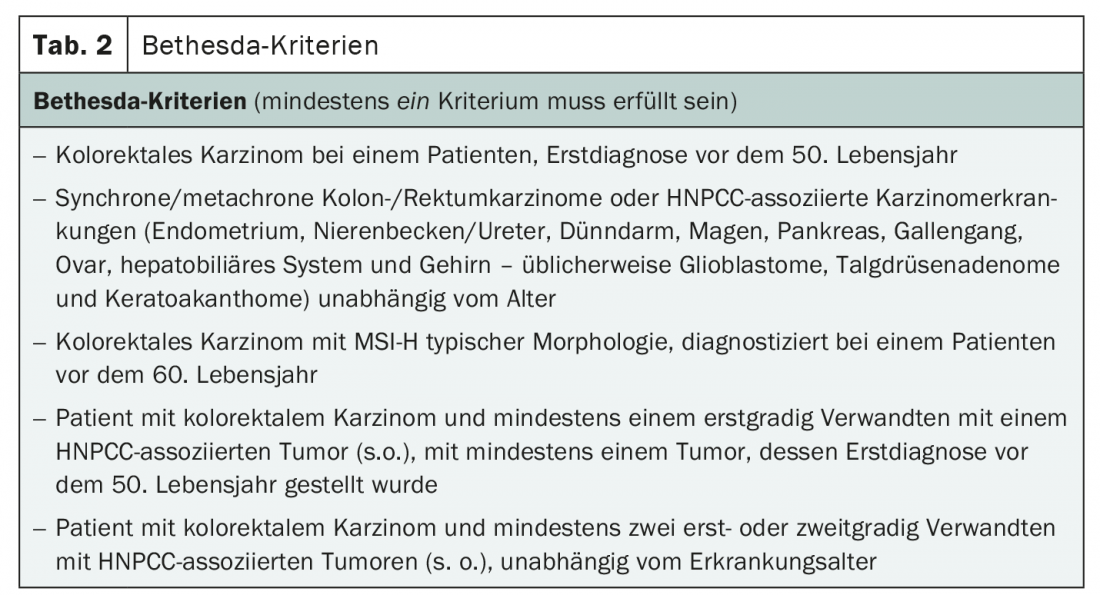
In 60% of cases, patients with a germline mutation fulfill the Amsterdam criteria (Tab. 1) . These are therefore also clarified in the first step of diagnostics. However, to cover the remaining affected individuals, the Bethesda criteria are also used as an indication for molecular genetic analysis of the tumor tissue (microsatellite analysis and immunohistochemical analysis) (Table 2) . If at least one criterion is met, further investigations should be performed. This includes a molecular pathological examination of the tumor tissue as well as molecular genetic studies of the blood. Treatment of Lynch syndrome usually consists of resection of the index lesion with regular search for other tumors. In the case of extensive tumor disease, chemotherapy is also administered.
Name giver Henry T. Lynch
As is so often the case, Lynch syndrome was named after its first describer, Henry T. Lynch. The American surgeon (1928-2019) was known for his discovery of familial susceptibility to certain cancers and his research into genetic links in cancer. Early in his career, he recognized that some cancer patients had relatives and ancestors who had the same type of cancer and postulated that cancer could be hereditary. He began to focus his research on this possibility, although it was considered unlikely by the medical establishment of the time. At the time, the focus was more on environmental causes of cancer. In 1970, he applied for a research grant citing a family in which numerous members had colon cancer. The application was rejected – as were most of his applications over the next 20 years. Nevertheless, he persisted and defined the necessary criteria for a genetic cancer: an early age of onset, a specific pattern of multiple primary cancers, and Mendelian inheritance patterns. Eventually, he was able to prove his theories. He demonstrated the Mendelian inheritance pattern for certain breast and ovarian cancers, laying the foundation for the identification of specific genes, such as BRCA1 and BRCA2. The best-known example, however, is the most common form of hereditary colorectal carcinoma: Lynch syndrome.
Further reading:
- www.hnpcc.de/lynch-syndrom.html
- www.mgz-muenchen.de/erkrankungen/diagnose/hereditaeres-nicht-polypoeses-kolonkarzinom-hnpcc-lynch-syndrom.html
- www.msdmanuals.com/de-de/profi/gastrointestinale-erkrankungen/tumoren-des-gastrointestinaltrakts/lynch-syndrom
- flexikon.doccheck.com/en/Lynch syndrome
- www.humangenetics.uni-bonn.de/de/beratung/erbliche-tumorerkrankungen/krankheitsbilder/hnpcc-lynch-syndrom
- https://en.wikipedia.org/wiki/Henry_T._Lynch
InFo ONCOLOGY & HEMATOLOGY 2022; 10(2): 36.









