Histamine intolerance (HIT) is a food intolerance that involves a series of adverse reactions as a result of accumulated or ingested histamine. It is caused by an imbalance between the amount of histamine released from food and the organism’s ability to break down this amount. Detecting a HIT, however, is not that easy.
Disturbed histamine breakdown can lead to numerous problems. Histamine intolerance (HIT) has therefore become the focus of increasing public attention in recent years. The question often arises for practitioners as to whether or when this condition should be taken seriously. HIT is the name for a food intolerance that includes a range of adverse reactions as a result of accumulated or ingested histamine. It is associated with decreased activity of the enzyme DAO, which leads to increased histamine concentration in plasma and the occurrence of adverse reactions [1]. HIT must be distinguished from histamine intoxication, which is also known as scrombroid syndrome, scombroidosis or histamine poisoning. The term derives from the name of the mackerel family (Scombridae) after whose consumption intoxication was most frequently observed. The family Scombridae includes tuna, herring and mackerel. Histamine poisoning is considered one of the most common poisonings caused by fish consumption worldwide [2]. In HIT, the amount of histamine ingested is much less than in histamine poisoning. Also, HIT manifestations are milder compared to intoxication.
Heterogeneous appearance
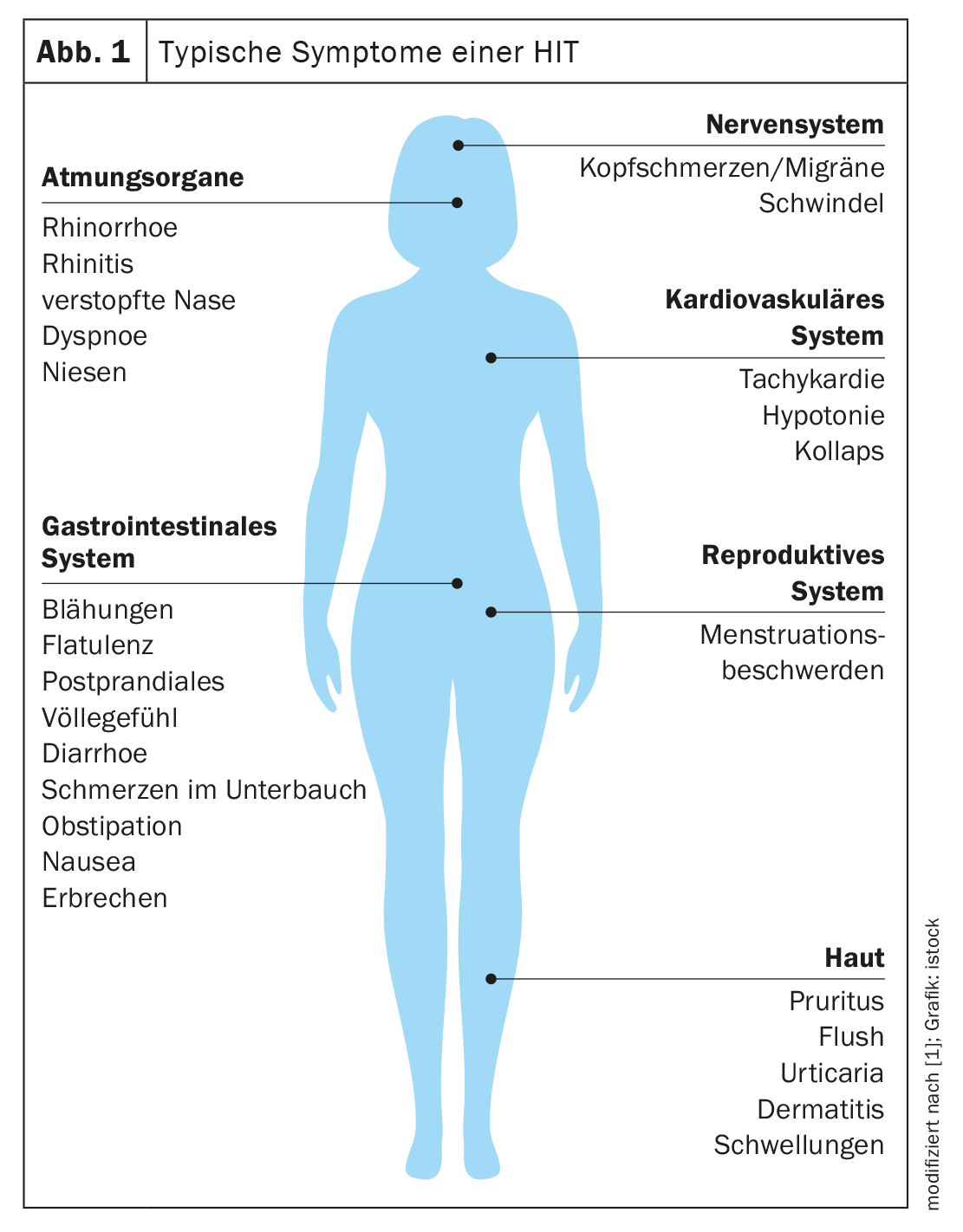
The manifestations of HIT can be caused by different pathophysiological mechanisms or a combination of them. The complex symptomatology is based on the fact that histamine receptors can be found in many organs of the body [1]. This shows a high diversity but also inconsistency of manifestations in one and the same person after similar stimuli. Typical signs include skin manifestations, e.g. redness on the face (flush), itching or urticarial rash on the body. Gastrointestinal symptoms include diarrhea but also constipation and abdominal pain. Manifestations in the cardiovascular system such as low blood pressure and tachycardia are observed, as are complaints in the nervous and respiratory systems. These include, for example, headaches, migraines, or dizziness (Fig. 1) [1,3].
Histamine content in the body
Whether symptoms appear depends on the histamine content in the body. Histamine is produced endogenously and stored predominantly in mast cells and basophils. Mast cells, basophils, enterochromaffin-like cells of the stomach, and histaminergic neurons are the best described cellular sources of histamine. However, other cell types, e.g. platelets, dendritic cells (DCs) and T cells, can also express histidine decarboxylase (HDC) after stimulation. HDC expression and histamine release are influenced by cytokines such as IL-1, IL-3, IL-12, IL-18, GM-CSF, macrophage colony-stimulating factor, and tumor necrosis factor (TNF)-α 1, 11, 12 [4].
Histamine affects the entire spectrum of physiological functions of various tissues and cells, including immunity [1,4]. From a chemical point of view, it is a ubiquitously occurring biogenic amine. In the organism, its synthesis is ensured by decarboxylation of the amino acid L-histidine by the enzyme L-histidine decarboxylase. Histamine acts in the organism as an agonist of histamine receptors H1, H2, H3 and H4 [1]. The different effects depend on the receptor subtypes and their differential expression (Table 1) [4]. H1 and H2 receptors occur ubiquitously, with H2 present primarily in the digestive tract (stomach, duodenum, small intestine). H3 receptors are abundant in the nervous system and H4 receptors are present in certain tissues (skin, tonsils), but in small amounts.
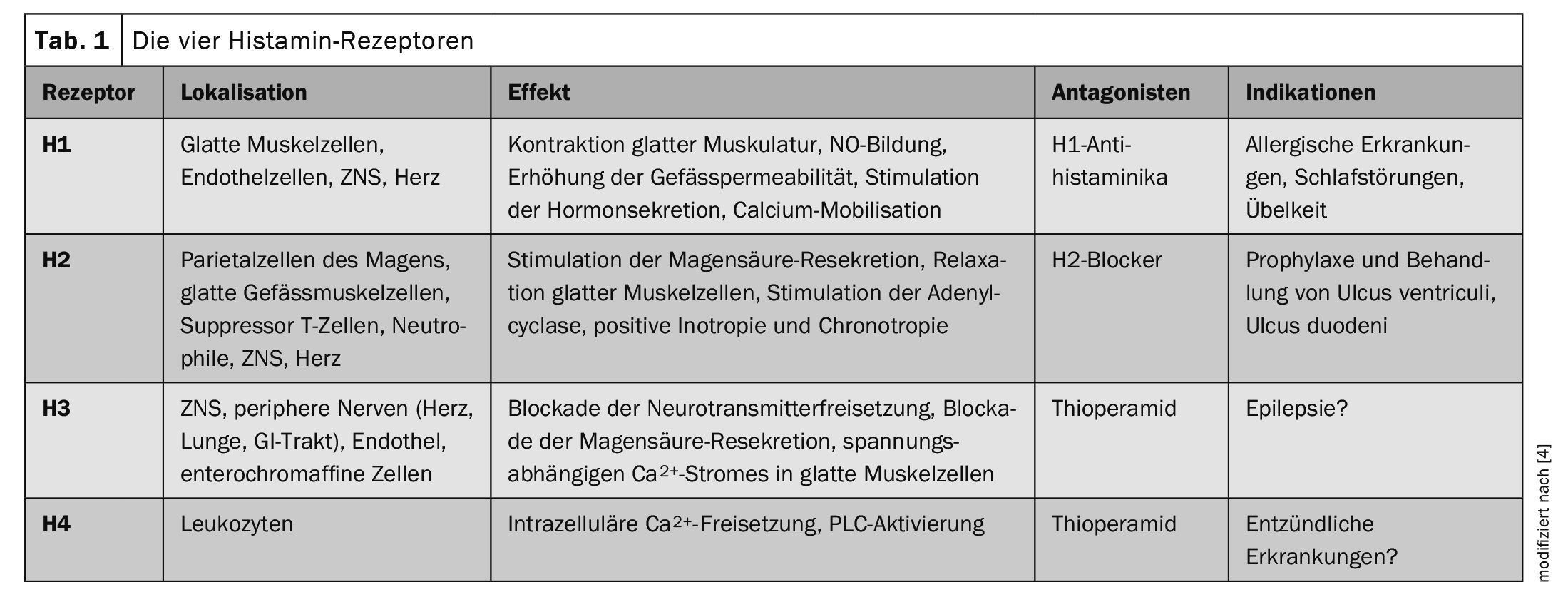
The H1 receptors are the best researched. They are expressed in many cells, including mast cells, and are involved in type 1 hypersensitivity reactions. Similar to H1R, H2R is expressed in a variety of tissues and cells, including the brain, gastric parietal cells, smooth muscle cells, T and B cells, and cardiac tissue. H2R can modulate a number of immune system activities such as mast cell degranulation, antibody synthesis, cytokine production, and T-cell polarization. H3R is a presynaptic autoreceptor in the peripheral and central nervous system and has been shown to be involved in sleep-wake rhythm, cognition, homeostatic regulation of energy levels, and inflammation. The H4R is the most recent receptor to be discovered and shares some molecular and pharmacological properties with the H3R. However, unlike H3R, H4R is expressed by a variety of cells, including keratinocytes, Langerhans cells, DCs, neutrophils, and lymphocytes [4].
Histamine degradation
Histamine is degraded by oxidative deamination (diamine oxidase, DAO) or by ring methylation (histamine N-methyltransferase, HNMT) [5]. DAO is stored in vesicular structures associated with the plasma membrane in epithelial cells and is secreted into the bloodstream after stimulation. Histamine N-methyltransferase, on the other hand, is a cytosolic enzyme that can convert histamine only in the intracellular space. Histamine N-methyltransferase is widely distributed in human tissues. The strongest expression is found in kidney and liver, followed by spleen, colon, prostate, ovaries, spinal cord cells, bronchi and trachea. Histamine N-methyltransferase is therefore also considered the key enzyme for histamine degradation in the bronchial epithelium [4,6]. In contrast, DAO expression in mammals is restricted to specific tissues such as small intestine, colon, placenta and kidney [5]. The physiological function of DAO enzyme includes regulation of inflammatory processes, proliferation, allergic reactions and ischemia [1]. The effect of DAO can be inhibited by alcohol and drugs.
Multidisciplinary diagnostics
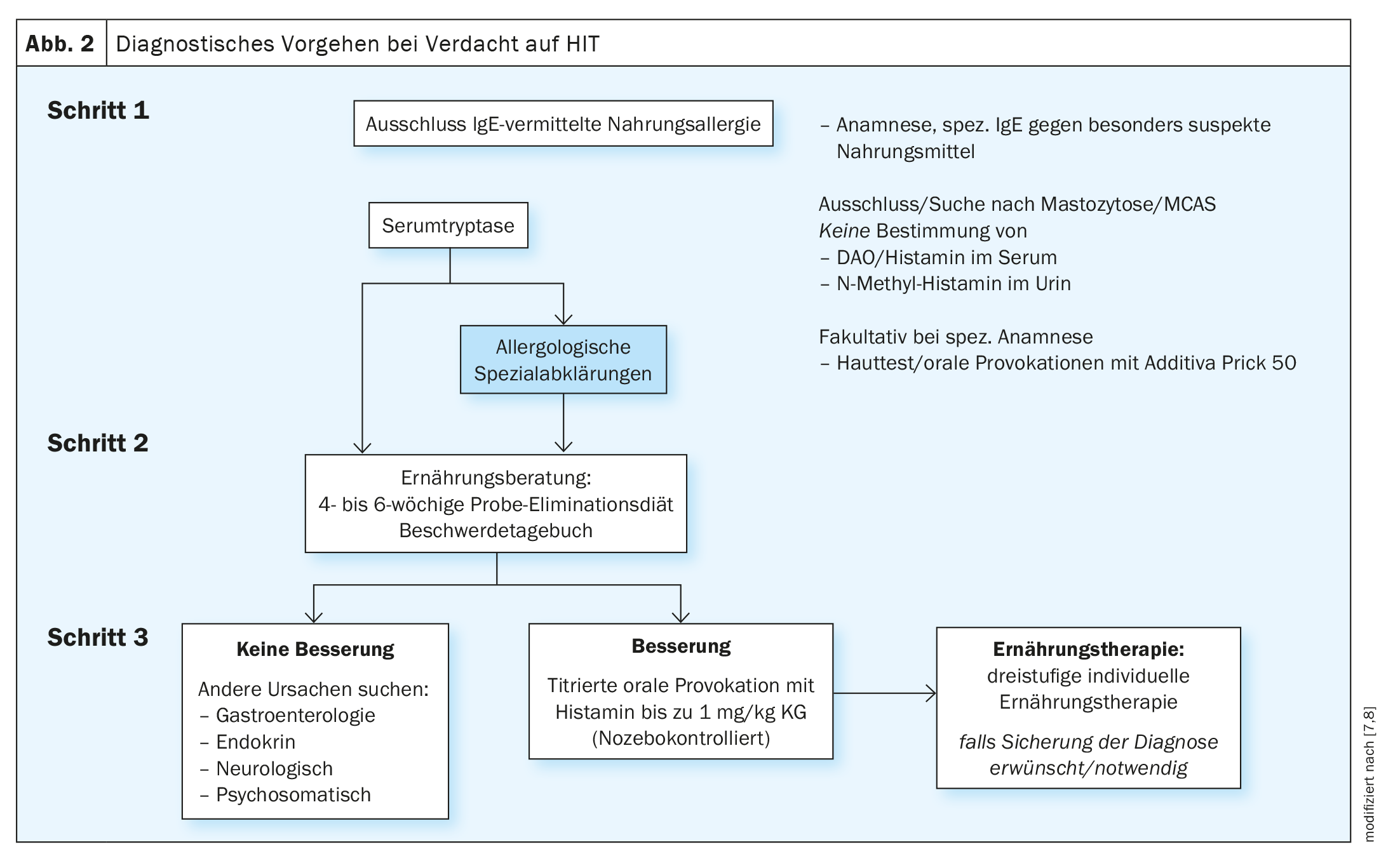
Diagnosis of HIT requires a complex and time-consuming multidisciplinary approach, including systematic elimination of diseases with similar symptoms (Fig. 2) [7,8]. HIT-specific diagnostic criteria or markers are lacking. The manifestation of HIT symptoms is thought to originate from decreased concentration/activity of DAO. On this basis, the measurement of the concentration or activity of this enzyme could be done for the diagnosis of HIT. The problem, however, is that a reference value for serum DAO levels has not yet been established. In addition, a measured DAO level and/or serum DAO activity may differ from the current level/functional activity of DAO in the intestinal mucosa. Currently, the exclusion of an actual IgE-mediated allergy is therefore sought as a sensible measure if the complaints can be associated with a specific food. With the help of skin tests, molecular allergy diagnosis and, if necessary, oral provocation tests for the food additives often suspected by patients, a well-founded allergological clarification can take place. In the second step, underlying mastocytosis should be considered. Here, the determination of serum tryptase can provide clues. Determination of the c-Kit mutation in the peripheral blood or a bone marrow examination can also help. In turn, the diagnosis of mast cell activation syndrome (MCAS) is based on response to H1R blockers and a significant increase in serum tryptase in the attack. If these measures still do not lead to a clear picture, an allergy-trained nutritionist should be consulted. An improvement of the symptoms under histamine reduction speaks for a HIT – at least as a co-factor. However, if there is no improvement or hardly any improvement, further investigations are indicated. This may be titrated oral histamine provocation, ideally double-blind and placebo-controlled with clinically defined parameters as endpoints. Here, histamine is added in increasing titration steps in amounts up to 75 mg – with inclusion of placebo doses. This should be done as part of an inpatient stay in combination with appropriate diet, nutritional counseling and, if necessary, other specialists from allergology, dermatology and psychosomatics. In Switzerland, this is offered at the Davos-Wolfgang High Mountain Clinic(www.hochgebirgsklinik.ch) as part of a hospitalization lasting several days. In many cases, a detailed gastroenterological examination should also be performed for the frequently occurring gastrointestinal complaints. However, hormonal or neurological diseases should also be considered, depending on the symptoms. Psychosomatic complaints can also rarely be ruled out completely – whether as a primary cause or as a result of the constant insecurity about eating.
Since histamine receptors (H1, H2 and especially H3 receptors) are present in the peripheral as well as in the central nervous system, histamine has a high impact on neuropsychological aspects. In addition, N-metnhyltransferase plays an essential role in the degradation of histamine in the CNS; therefore, in addition to the migraine already mentioned, other diseases such as Parkinson’s disease, ADHD or myasthenia gravis are also associated with altered function of this enzyme. Since various drugs such as chlorquine inhibit N-methyltransferase, the neuro-psychological effects and symptoms of histamine can be enhanced by corresponding drugs [9,10].
That psychosomatic factors may be involved is also shown from another side in the fact that placebo-controlled provocations a not inconsiderable proportion of the patients also experience complaints in response to the placebo alone, as with the ingestion of histamine-containing products. The expectation that histamine-rich foods trigger discomfort can therefore also be “burned in” mentally – especially if this experience has been made so several times. Since factors influencing histamine degradation, such as the microbiome, can change, a gradual attempt to relax dietary measures is certainly justified, especially under expert nutritional advice.
Therapy management of HIT
Among therapeutic approaches, the gold standard is a low-histamine diet. A good response to such a diet is considered a confirmation of HIT. In addition to dietary measures, DAO supplementation, which supports the breakdown of ingested histamine, may be considered as an adjunct treatment for individuals with intestinal DAO deficiency. The use of H1R-targeted antihistamines may also be useful.
Low histamine diet: The principle of the low histamine diet is to select foods that are not expected to contain excessive amounts of histamine or biogenic amines. It is divided into three phases: Karenzphase, test phase and Dauerernährung. In the first phase, foods that typically contain a high amount of histamine should be completely excluded. There is wide variation among studies in the types of foods that should be avoided during the elimination diet. Some of the routinely excluded foods contain only small amounts of biogenic amines and are referred to as histamine releasers [11]. The focus should be on a mixed vegetable diet for ten days to three weeks, with foods consumed as fresh as possible. After that, the test phase follows for about six weeks, during which targeted suspicious foods are reintroduced. In the phase of permanent nutrition, individual eliminations should be used to achieve nutrition that meets the patient’s needs while maintaining a high quality of life. Often, sufferers already benefit by changing the combination of the main food groups protein, fat, carbohydrates or/and by changing the meal structure.
Supplementation of DAO: Similar to the use of lactase supplementation in lactose intolerance, exogenous delivery of DAO enzyme has been developed for HIT [1]. A porcine kidney extract containing 0.3 mg DAO enzyme may be administered as a food for special medical purposes. The maximum daily dose of exogenously ingested enzyme is 3× 0.3 mg, which corresponds to 0.9 mg DAO. Clinical practice has shown that exogenous supplementation of DAO can significantly improve symptoms in a proportion of patients. Supplementation with vitamin C (100-1000 mg/day), vitamin B6, or copper may additionally be considered, as these substances promote the degradation of histamine via DAO or HNMT.
Antihistamines: Treatment of patients with antihistamines is empiric. There are no randomized clinical trials demonstrating the contribution of this therapy in HIT. However, considering efficacy and safety, second- or third-generation H1 antihistamines should take precedence. H2 blockers could be used in patients with dominant gastrointestinal symptoms. Treatment with antihistamines should be deliberate and time-limited, and should help to form a picture of whether H1/H2 receptor blockade attenuates manifestations. Accordingly, they can also be used as a therapeutic diagnostic test [1].
Conclusion
HIT is a variety of different symptoms that occur after the consumption of histamine-rich foods. The manifestations may be caused by different pathophysiological mechanisms or a combination of them. Therefore, the diagnosis of HIT requires a complex and time-consuming multidisciplinary approach, including the systematic elimination of diseases with similar symptoms. A low-histamine diet is currently a suitable (but not the only) diagnostic and at the same time therapeutic measure. In addition to dietary measures, oral DAO supplementation and the use of H1R-targeted antihistamines may be targeted [12].
Take-Home Messages
- HIT is a food intolerance that involves a series of adverse reactions as a result of accumulated or ingested histamine.
- It is caused by an imbalance between the amount of histamine released from food and the organism’s ability to break down this amount.
- Symptoms range from gastrointestinal discomfort to sneezing, difficulty breathing, flushing, itching, headache or dizziness.
- The diagnosis should be multidisciplinary and the systematic
Include elimination of diseases with similar symptoms. - A gradual, low-histamine diet, oral DAO supplementation, and administration of H1R-targeted antihistamines may help relieve symptoms in patients with HIT.
Literature:
- Hrubisko M, Danis R, Huorka M, Wawruch M: Histamine Intolerance – The More We Know the Less We Know. A Review. Nutrients 2021; 13(7): 2228.
- Colombo FM, Cattaneo P, Confalonieri E, Bernardi C: Histamine food poisonings: A systematic review and meta-analysis. Crit Rev Food Sci Nutr 2018; 58: 1131–1151.
- Reese I, Ballmer-Weber B, Beyer K, et al.: German guideline for the management of adverse reactions to ingested histamine. Allergologie 2021; 10:761-772.
- Smolinska S, et al.: Histamine and gut mucosal immune regulation. Allergy 2014; 69(3): 273-81.
- Klocker J, Matzler SA, Huetz GN, et al.: Expression of histamine degrading enzymes in porcine tissues. Inflamm Res 2005; 54(Suppl 1): S54–S57.
- Yamauchi K, Sekizawa K, Suzuki H, et al.: Structure and function of human histamine N-methyltransferase: critical enzyme in histamine metabolism in airway. Am J Physiol 1994; 267(3 Pt 1): L342–L349.
- Reese I, et al.: Guideline on management of suspected adverse reactions to ingested histamine: Guideline of the German Society for Allergology and Clinical Immunology (DGAKI), the Society for Pediatric Allergology and Environmental Medicine (GPA), the Medical Association of German Allergologists (AeDA) as well as the Swiss Society for Allergology and Immunology (SGAI) and the Austrian Society for Allergology and Immunology (ÖGAI). Allergol Select 2021; 5: 305–314.
- Tuck CJ, Biesiekierski JR, Schmid-Grendelmeier P, Pohl D: Food Intolerances. Nutrients 2019; 11(7): 1684.
- Sergeeva OA, Klyuch BP, Fleischer W, et al: P2Y receptor-mediated excitation in the posterior hypothalamus. Eur J Neurosci. 2006 Sep; 24(5): 1413-1426.
- Yoshikawa T, Nakamura T, Yanai K. Histamine N-methyltransferase in the Brain. Int J Mol Sci. 2019 Feb 10;20(3):737.
- Sánchez-Pérez S, Comas-Basté O, Veciana-Nogués M, et al.: Low-histamine diets: Is the exclusion of foods justified by their histamine content? Nutrients 2021; 13: 1395.
- Schmid-Grendelmeier P , Gianelli D, Gutzweiler JP, et al.: Histaminintoleranz – zwischen Mythen und Fakten. Schweizer Zeitschrift für Ernährungsmedizin 2022; 2: 10–15.
InFo NEUROLOGIE & PSYCHIATRIE 2023; 21(3): 6–10