For a long time, it was not clearly established whether diabetics are generally suitable for driving a vehicle or not. With the adoption of the S2e guideline “Diabetes and Road Traffic”, legal certainty was created for physicians for the first time.
Participation in road traffic in Switzerland is regulated by the Road Traffic Act. This states that motor vehicle drivers must be fit and competent to drive. As the guideline states, fitness to drive is understood to mean the ability to drive a motor vehicle in road traffic that is largely stable over time and independent of current situation and state of mind parameters. Physical and psychological characteristics can have a detrimental effect here. There has long been debate about whether patients with diabetes are fit to drive. Particularly with regard to professional drivers, it has often been argued that insulin-dependent patients should be denied a driver’s license.
The guideline has put the assessment of fitness to drive in diabetes on a medical-scientific footing. For example, the results of a 2016 meta-analysis show that the risk of accidents is increased by only about 11% for people with diabetes – much lower than the risk for people with sleep apnea syndrome (140%) or attention-deficit/hyperactivity disorder (340%). Analyses suggest that the disease per se is not associated with an increased risk of accidents. Accordingly, almost all diabetes patients can participate in road traffic, both in private cars and professionally. However, high-risk groups have been identified within the disease where the risk assessment is significantly worse.
High long-term blood sugar is not a reason for driving ban
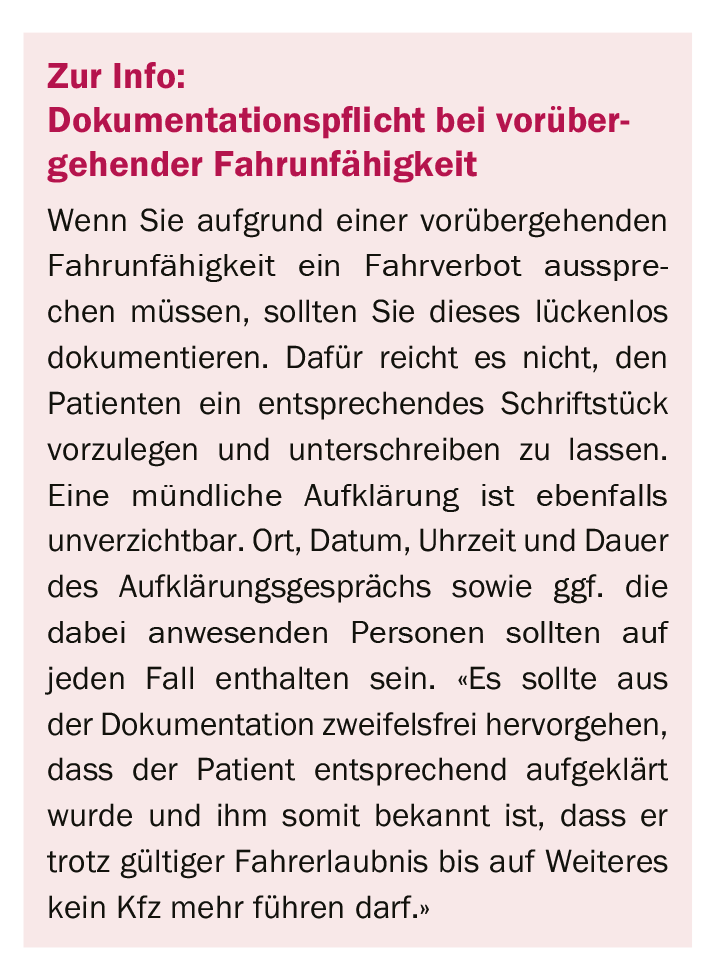
While a high HbA1c level or insulin therapy are not grounds for banning driving, caution should be exercised with two or more episodes of severe hypoglycemia while awake within a year or untreated sleep apnea. Comorbidities should also be kept in mind. Temporary incapacity to drive occurs, for example, in the case of severe metabolic derailments or during the phase of adjustment to insulin or dose adjustments. In this case, it is necessary to wait until the blood glucose metabolism is stable again.
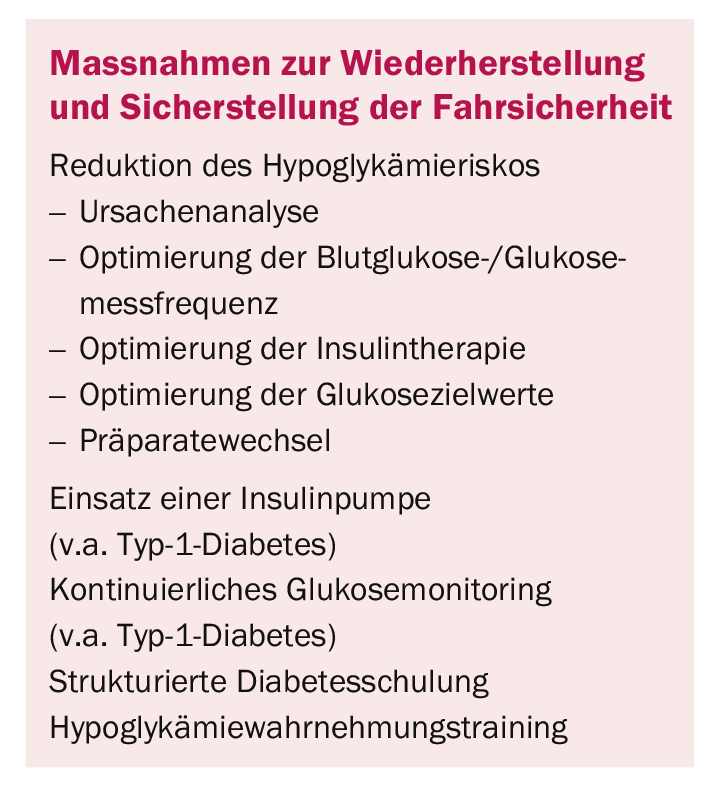
The top priority should, of course, be to avoid hypoglycemia. Accordingly, the patient is advised to perform a blood glucose self-monitoring before starting a journey. In addition, fast-acting carbohydrates such as glucose or similar should always be available in the vehicle so that the blood glucose can be raised in a targeted manner if necessary.
According to an initial assessment, the guideline has provided (legal) certainty for patients, physicians and even experts. Structuring through clear criteria based on scientific findings leaves less room for interpretation and provides comprehensible recommendations for action.
CARDIOVASC 2019; 18(3): 34