Whether structured, organized and performance-oriented sport is a positive thing already in childhood is today judged very controversially (keyword: early specialization vs. general training). The fact is that in many sports (football, gymnastics) this form of early training is practiced. That’s why it’s worth thinking about the connections between growth and performance sports.
In most sports, children are divided into year levels. At first glance, this seems like a logical decision, since children at roughly the same stage of development can compete in a fair way. This at least is the wish, which unfortunately cannot always be realized in practice.
From a certain level of performance, it is not uncommon for clubs to require young people to undergo a sports medical examination, even though this procedure is not mandatory in Switzerland, unlike in some neighboring countries. This preventive health checkup involves anthropometric measurements such as height, weight, and skinfold measurement (or bioimpedance). Often, these values are plotted on growth curves to monitor progress and are presented and explained to the adolescent’s parents with the overall results of the check-up. At extreme values (3rd and 97th percentiles), this poses a problem for the sports physician that cannot be trivialized.
The differences compared to adults
How to act if the parents have not yet dealt with this problem? Or the pediatrician addressed did not perceive the important connections between growth and (competitive) sports, which is not uncommon? Should you get a wrist x-ray (of the non-dominant side!) right away? Or have the growth hormone level determined?
It cannot be reminded often enough that a child is not a miniature adult, so it differs from adults not only quantitatively but also qualitatively. The explanation for this is the growth that takes place, which involves numerous physical, psychological as well as psychosocial changes and peculiarities of development. This situation implies corresponding consequences for physical and sporting activities.
Consider the centripetal regularity
Another important argument is the fact that human growth varies individually and is not linear in any way. It depends on the size of the parents (genetic factors), nutrition, hormones, as well as the environment. Phases of rapid growth (first year of life, puberty) alternate with slow growth (preschool age). The growth is finished with the closing of the growth plates. The increase in size is identical to the increase in weight and the development of the individual organ systems. It is essential for athletic activity that the individual body segments grow at different intensities. This changes the body proportions, an aspect relevant to athletic performance. The peculiarity of the growth spurt during puberty is the different development of individual skeletal sections: Feet and hands mature earlier than lower legs and forearms, and these in turn earlier than thighs and upper arms. This phenomenon is called centripetal regularity.
Discrepancy between calendrical and biological age
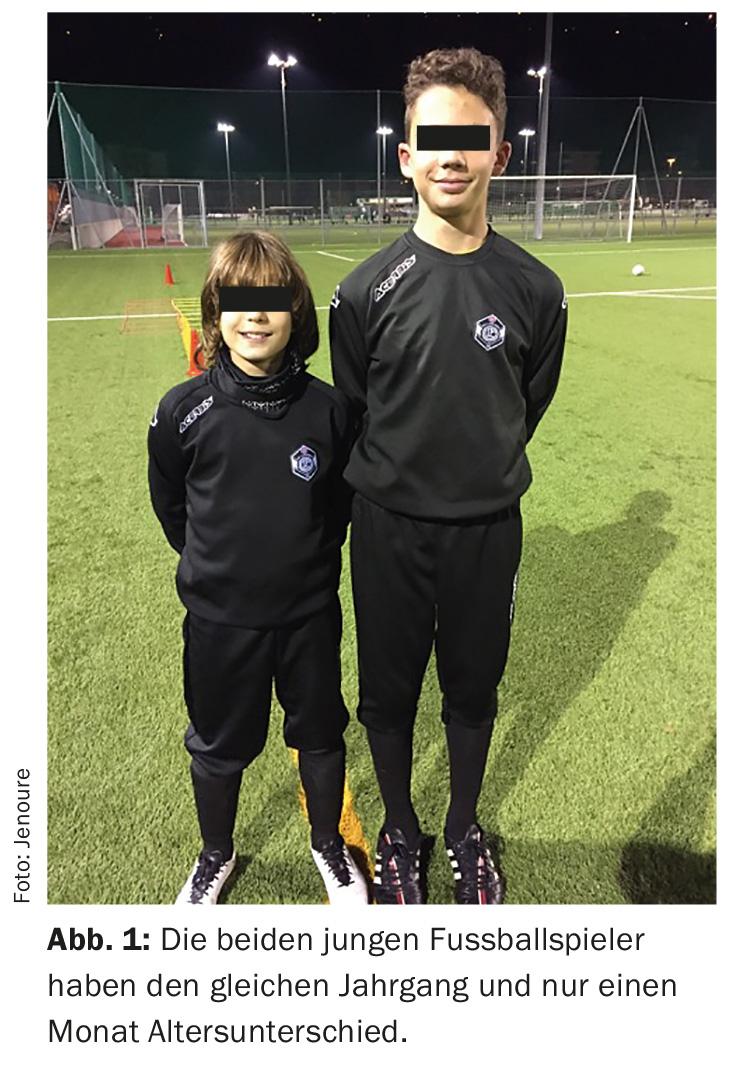
When it comes to growth and sport, however, there is an issue that is even more essential: that of the frequently encountered discrepancy between calendrical and biological age. The literature refers to this as acceleration and retardation, respectively, although the term deceleration is preferable because it does not give the impression of anomaly. In a normally developing child, the calendrical and biological ages coincide; an early-developing, i.e. accelerated, child has a higher biological age than calendrical age, while the opposite is true for the late-developing child. In extreme cases, these variations can account for up to five years between two young people with almost the same date of birth. Imagine what happens on the sports field when such diverse young people who play sports in the same category “collide.”
Not to be forgotten is the fact that in addition to the morphological acceleration, which is the most visible, there is also a functional one: Athletic performance also increases globally (aerobic and anaerobic capacity, strength, speed). In all types of development, however, harmonious global growth is the rule, also in terms of performance. Further, these developmental differences and sport are clearly interrelated. Besides the mentioned effect, a regular physical training also favors a synchronization of the maturation process. The once determined difference between bone age and calendrical age therefore does not remain identical over time! Sport once again proves to be an excellent therapy for adolescents who show disharmonious developmental trajectories, mostly non-athletic adolescents.
Unfavorable comparisons with early developers
These findings clearly show that the division of age groups in children’s sports, at school or in clubs, according to calendar age is anything but unproblematic. Any objective assessment and evaluation (grades) quickly proves difficult or even impossible, and harmful and counterproductive if the clear findings are not taken into account. Many talents have been lost to the sports world because they were unfairly compared unfavorably to early developers in their age group. This led them to become disgusted with the sport. Those who are more capable, on the other hand, run the risk of overstimulating their apparent talent too early with training methods that are not age-appropriate (mostly from adult sports).
An X-ray can bring help
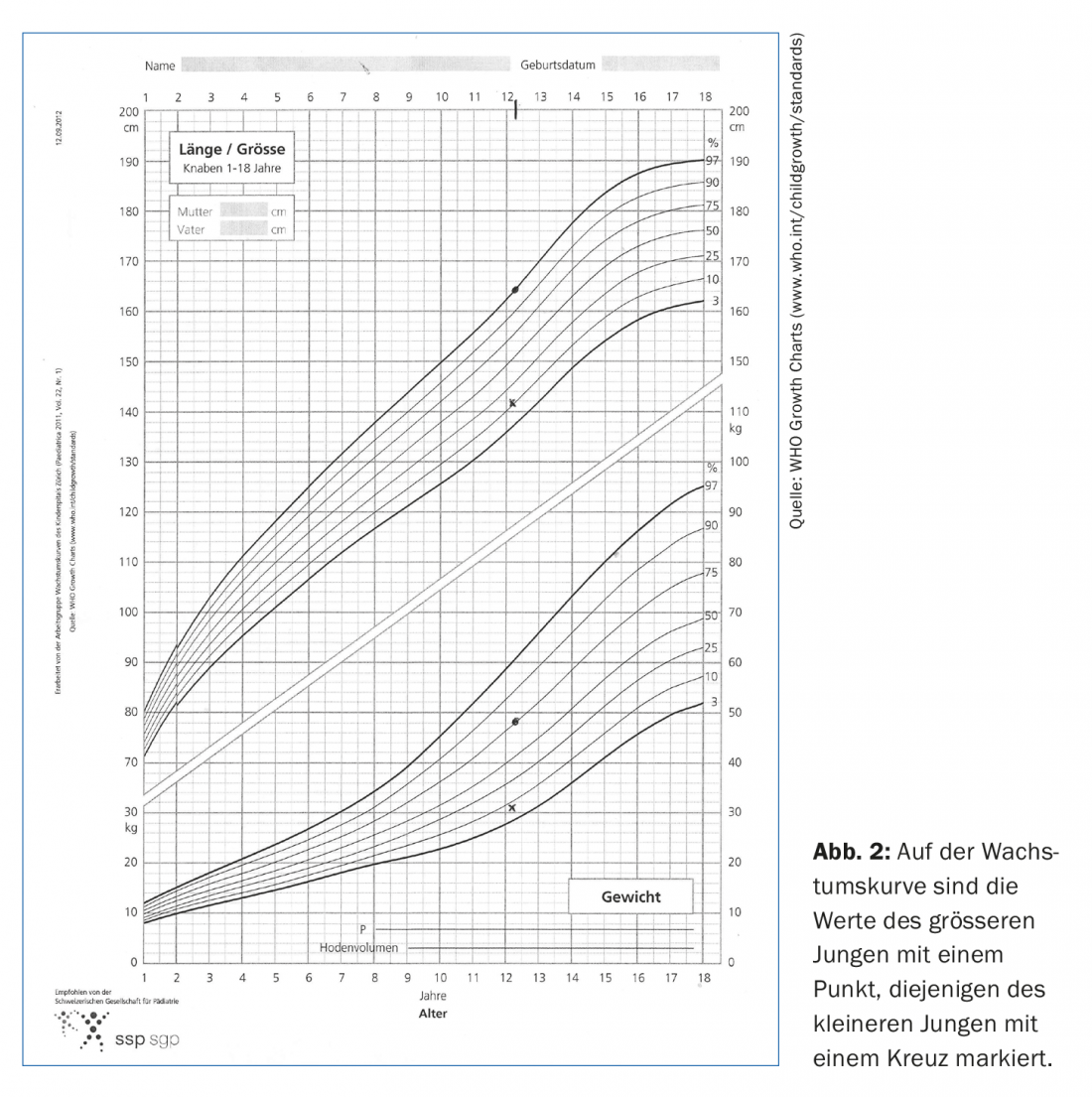
Back to the question asked at the beginning of the sports medical examination: what to do with a child who has a height between the 3rd and 10th percentiles? It is not easy to answer this question conclusively. The first thing to do is to put body size and weight in relation to each other (Figs. 1 and 2). If there is harmony, all the better. It is also possible to ask the treating pediatrician how he or she assesses the situation, and it is helpful if previous measurement data are available. If the growth line does not cross a percentile line, this also tends to be a positive sign that there is no growth disorder. However, our experience shows that pediatricians often take too little account of the “athletic” situation: Between the 3rd and 97th percentiles, a point is normal, but a size below the 10th percentile can put a young ambitious athlete at a real disadvantage.
An X-ray of the wrist could bring help. In the atlas method according to Greulich and Pyle, the X-ray image of the left hand is compared with reference images from an atlas. The skeletal age is derived from the image that is closest to the current image. Somewhat more differentiated and more frequently used in Germany is the method according to Tanner and Whitehouse. Several images are used and point values are assigned. In addition to the carpal bones, the ulna and radius as well as selected metacarpal bones and phalanges are also included. Possibly with a slightly higher radiation exposure.
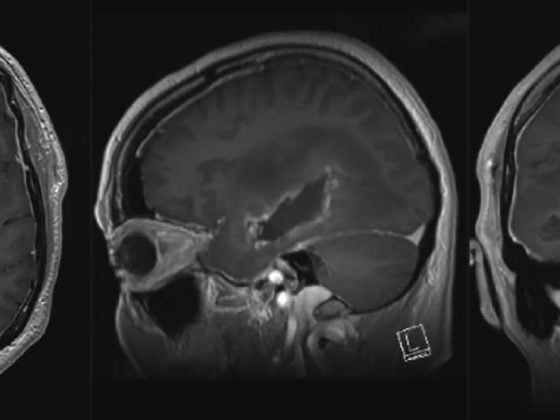
Further clarifications by the specialist
Speaking of radiation exposure, it is interesting to note that FIFA has developed a now validated method using MRI of the wrist! Our justification of the X-ray is the fact that the medical commission of the Swiss Football Association SFV has issued exemption permits in the elite field for late developers. If the height deviation is 2 SD below the 50th percentile and there is a difference of one year between the calendar age and the bone age, the young person can play in the lower category after approval of a corresponding request. Depending on interest, knowledge, and time, one may still inquire about the final height of the biological parents and/or anamnestic information such as pelvic position at birth, the presence of hypoglycemic episodes during the neonatal period, the child’s eating behavior, and the preexistence of illness.
This is important information for the initiation of further clarification, but it is usually left to the specialist. Further, growth and pubertal progression of parents and siblings should be inquired in order to shed more light on the genetic potential. The determination of growth hormone and other complex blood parameters should be left to the specialist if it is really a matter of investigating the (strong) suspicion of a growth disorder. However, this situation is rarely found among athletically talented young people!
Checking the growth of his young athletes is also an important task for the sports physician. Unlike for the pediatrician, the issue of performance in relation to growth almost comes to the forefront for him. It is therefore important for the sports physician to be informed about these mentioned findings.
HAUSARZT PRAXIS 2017; 12(1): 5-6