
Impaired wound healing in diabetic patients is a problem with increasing frequency, which causes enormous costs and is still largely unsolved. An overview of pathogenesis.
Despite the undoubted progress in the treatment of diabetes and its sequelae, the problem of microvascular complications and especially diabetic foot ulcers remains a major challenge for patients and medical staff. Microvascular complications are also increasing worldwide due to the success in the treatment of macrovascular complications and the associated improvement in life expectancy [1]. Epidemiological figures from Switzerland are difficult to obtain, but it can be assumed that we have comparable results with the other European countries. Based on data from the UK, Germany or the USA, it can be assumed that the number of amputations in diabetic foot syndrome has not decreased in recent years and that, at best, the level of amputation has improved [2].
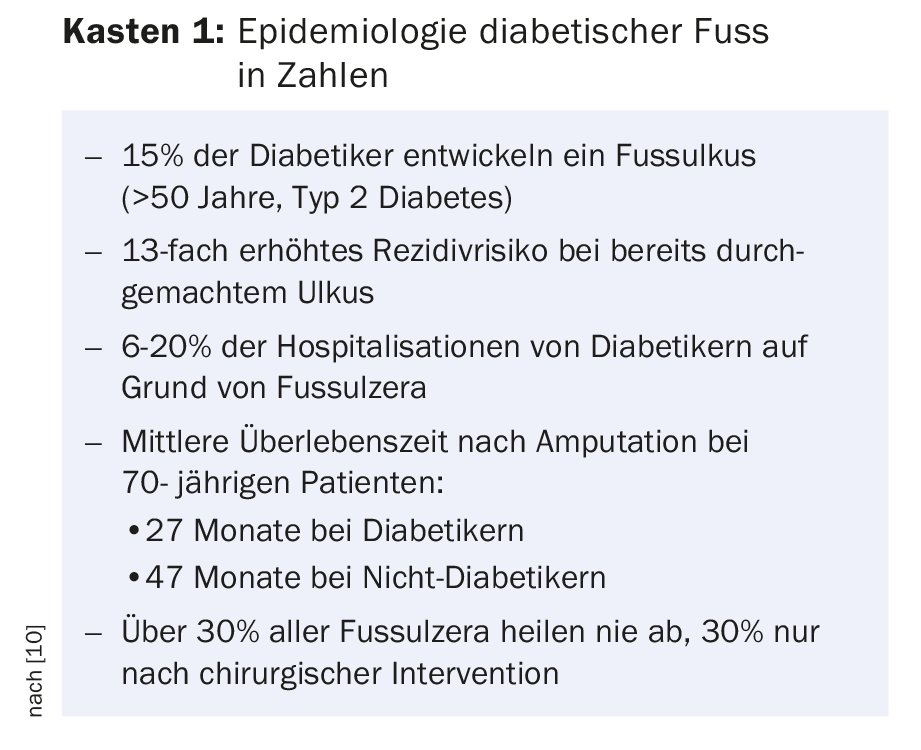
Furthermore, the figures also show that significantly better results are achieved at highly specialized centers than the overall average. Nevertheless, it must still be assumed in 2018 that the problem of diabetic foot has not diminished and that no therapy is in sight in the foreseeable future to bring about a decisive improvement here. Diabetic foot syndrome and the resulting follow-up costs must still be considered the most expensive complication of diabetes, with mortality rates comparable to pancreatic or bronchus carcinoma (see Boxes 1 and 2) [3]. This article is mainly devoted to the problem of impaired wound healing in diabetic foot syndrome.

Etiology and pathogenesis
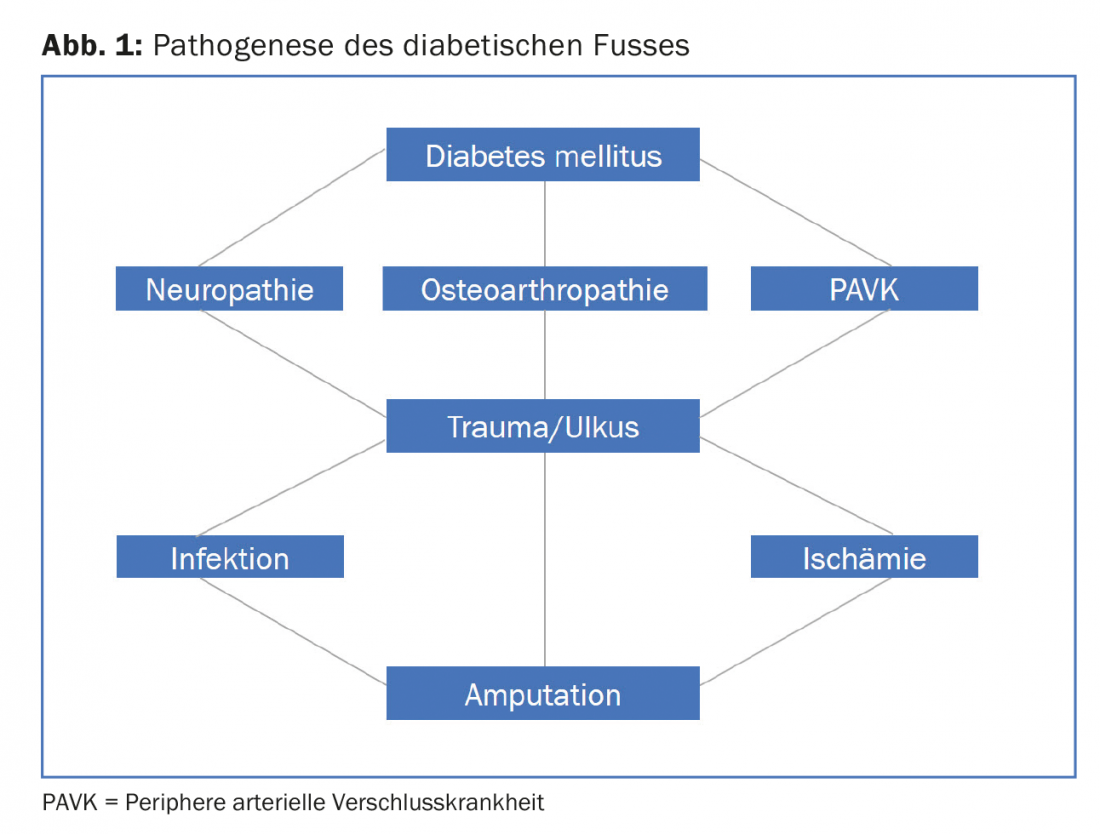
The pathophysiology leading from hyperglycemia to foot ulcer results from a complex, dysfunctional interplay between multiple, dysfunctional systems. In the previous medical view, it was mainly ischemia, repetitive trauma, and infection that were considered the main problems of recurrent chronic wounds. Treatment revolved primarily around wound care and revascularization (Fig. 1). Only in recent years has the disruption of the wound healing process in the skin itself been recognized as the main cause of wound healing disorder, and wound healing itself has been identified as another biological system disrupted by the metabolic, microvascular, neurological, and inflammatory changes that are typical of diabetes [4].
As a result of these findings, much research has been conducted with the primary goal of restoring the molecular and cellular processes in the wound that are necessary for successful wound healing.
Physiology of wound healing
Tissue injury triggers an acute inflammatory response characterized by the arrival of neutrophils, macrophages, and mast cells. These cells produce inflammatory cytokines and growth factors that coordinate wound healing. Complication-free wound healing requires a sequential and self-limiting cytokine-immune cell interaction to elicit an adequate immune response necessary for bacterial clearance, organized tissue breakdown, and subsequent tissue regeneration.
Systemic and local inflammation in diabetes
Type II diabetes mellitus is characterized by insulin resistance and accelerated atherosclerosis. Their common cause is chronic, low-threshold inflammation maintained by various cell mediators, including immune cells and adipocytes – including various pro-inflammatory cytokines as well as Il 1, INF alpha, Il 6. These inflammatory signs are significantly correlated with insulin resistance markers, HbA1c, lipid profile, hypertension, and physical activity, which is detectable in both type II and type I diabetes. This systemic inflammation correlates closely with local inflammation in that high glucose concentrations stimulate leukocytes to release proinflammatory mediators. This creates a distinct imbalance of pro- and anti-inflammatory cytokines, which are released in a non-sequential order, leading to impaired tissue repair and weakened cellular and humoral immune defenses [4,5].
In addition to the chronic damage caused by hyperglycemia, acute high glucose concentrations also trigger a change at the cellular level – as has been repeatedly shown in vitro, so that glucose concentrations as close to normal as possible should also be aimed for during the wound healing phase [6].
Neuropathy and wound healing
Diabetic neuropathy is a common, usually long unrecognized, long-term complication of the disease characterized by progressive loss of somatic and autonomic nerve fibers. Autonomic neuropathy results in anhydrosis, which leads to altered neurogenic regulation of cutaneous blood flow, making the skin dry and prone to cracking and fissuring. Somatic diabetic neuropathy, which occurs in up to 50% of patients depending on the duration of diabetes, is the most common and sensitive predictor of foot ulceration. Peripheral sensory neuropathy is the main culprit for foot amputations (Fig. 2) and increases the risk of foot amputation by 1.7-fold and by 36-fold with a history of ulceration [7].

Thus, diabetic neuropathy not only causes the foot wound to develop, but the wound is noticed too late due to the lack of pain sensation and is subjected to repetitive trauma over a long period of time, which further reduces the chance of wound healing (Fig.3). (Healing of acute wounds is not usually impaired in diabetic patients).

Delayed infection treatment
Due to the reduced expression of the inflammatory reaction in the context of neuropathy, both the patient and the attending physician often underestimate the danger situation, since the classic signs of inflammation are hardly present or significantly reduced due to the autonomic neuropathy and the microcirculatory disturbance. Due to the history, which usually lasts several weeks, extensive bacterial colonization or infection has then already occurred, not infrequently with pre-existing osteomyelitis (Fig. 3). This is also often misdiagnosed or mistaken for Charcot foot due to decreased systemic and local signs of inflammation over time [8].
Insufficient pressure relief
Another problem with wound healing in the presence of neuropathy is inadequate pressure relief. Although some form of pressure relief is usually sought in diabetic foot syndrome, this is not helpful in many cases and may even be counterproductive if necessary, causing additional pressure ulcers such as with an ill-fitting plaster cast or a shoe fitting whose appropriateness has not been verified by dynamic pressure measurement. As before, more than half of all poorly healing wounds are probably caused by inadequate infection treatment, lack of regular debridement and inadequate pressure relief [9].
Interdisciplinary team and patient education
Because of the many problems associated with diabetic foot wounds and the far-reaching consequences for those affected, care in an interdisciplinary team is strongly recommended. In this setting, it is often much more successful to optimally coordinate the therapy of factors that can currently be influenced, such as circulation, infection treatment, debridement, and pressure relief, and thus to achieve better healing rates. An important factor is the high recurrence rate and therefore the most promising intervention for diabetic foot syndrome in 2018 remains primary and secondary prevention [10].
Outlook
All attempts to intervene in the disturbed wound healing with local substances have so far been largely unsuccessful. A combination of growth factors and immunopeptides could be significantly more effective than the current monosubstances. Again, the problem of rapid degradation by proteases in the wound environment remains. Another theoretical approach is the application of protein-based substances introduced into the wound by viral vectors and gene therapy [4]. However, until initial results are available here, most patients with diabetic wounds are likely to have the best chance of healing in the hands of an interdisciplinary team.
Take-Home Messages
- Impaired wound healing in diabetic patients is a problem that is steadily increasing in frequency, causes enormous costs, and is still largely unsolved.
- Research in recent years shows profound disturbances at the molecular level (neuropeptide/immune axis) that go beyond the previously known factors of microcirculation, pressure load, and impaired defense against infection.
- Interdisciplinary teams have the greatest success rates, yet 30% of all ulcers heal only after amputation and 30% do not heal at all (11).
- DFS is only ever in remission, recurrence rates are high, and lifelong close monitoring of patients at risk is necessary (primary and secondary prevention).
- Local substances to improve impaired wound healing have so far been without demonstrable success; debridement, systemic infection treatment, and moist wound care remain the most important factors for successful wound therapy.
Literature:
- Centers For Disease Control And Prevention, et al: National diabetes statistics report: estimates of diabetes and its burden in the United States, 2014. Atlanta, GA: US Department of Health and Human Services, 2014.
- Prompers L, et al: High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe: baseline results from the Eurodiale study. Diabetologia 2007; 50: 18-25.
- Skrepnek GH: Health care service and outcomes among an estimated 6.7 million ambulatory care diabetic foot cases. Diabetes Care 2017; dc162189 (Epub ahead of print).
- Pradhan L, et al: Inflammation and neuropeptides: the connection in diabetic wound healing. Expert reviews in molecular medicine 2009; 11.
- Ridker PM, et al: Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease (Cantos Trial). NEJM 2017; 377(12): 1119.
- Wong Siu L, et al: Diabetes primes neutrophils to undergo NETosis, which impairs wound healing. Nature medicine 2015; 21(7): 815.
- Volmer-Thole M, et al: Neuropathy and Diabetic Foot. Int. J. Mol. Sci. 2016; 17: 917.
- Lipsky BA, et al: Infectious Diseases Society of America. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis 2012; 54: e132-e173.
- Bus SA, et al: Footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in patients with diabetes: a systematic review. Diabetes Metab Res Rev 2016; 32(1): 99-118.
- Amstrong DG, et al: Diabetic foot ulcers and their recurrence. N Engl J Med 2017; 376: 2367-2375.
- Armstrong DG, Harkless LB: Outcomes of preventative care in a diabetic foot specialty clinic. J Foot Ankle Surg 1998; 37: 460-466.
DERMATOLOGIE PRAXIS 2018; 28(1): 21-24









