
Gastric cancer often occurs in middle and later adulthood. More than 90% of gastric malignancies are adenocarcinomas; localized gastric lymphomas and leiomyosarcomas are less common. MRI can be used to differentiate various morphologic forms of adenocarcinoma. CT has little significance for diagnostic purposes, but is often used for tumor staging.
Numerous pathologic changes as causes of dysphagia have already been discussed as part of this series in Family Practice 2022. In addition to the localization of space-occupying lesions with consecutive dysphagia in the hypopharynx, larynx, and esophagus, as well as processes externally obstructing the passage of food, this article focuses on gastric carcinoma.
The incidence and lethality of gastric carcinoma have decreased in recent years. The rate of annual new cases in Germany in 2007 was 19 400, and the proportion of men was 11 200 [7]. 85% of malignancies were adenocarcinomas. Although located in the middle section of the digestive organs, the tumorous changes of the stomach may well develop an obstructive effect on the passage of the food pulp and dysphagia. Overview 1 lists the various symptoms [1] that may emanate from gastric carcinoma.
In the initial stage of gastric carcinoma, no or only minor, uncharacteristic symptoms are found. These are often ignored or misinterpreted as harmless food intolerances. Gastric carcinoma is frequently seen in middle and later adulthood [5]. The superficial form is rather rare. Chronic pre-existing conditions may favor the development of malignancy [2], such as pernicious anemia [3] and Menetrier’s disease [4]. This is atrophic gastritis with megaloblastic anemia or vitamin B12 deficiency anemia. Menetrier’s disease is giant fold gastritis. Gastric ulcers occasionally occur. The diagnosis is made histologically in both cases.
Adenocarcinoma is the most common tissue type [6]. In this context, infections with Helicobacter pylori have also been shown to be a promoting factor.
Radiographs play no role in the diagnosis of gastric cancer. In the past, double contrast examination of the stomach in hypotension was the primary imaging test to detect tumorous processes and functional disorders of the stomach. After the introduction of endoscopy, this imaging method no longer plays a role. In principle, endoscopy is considered the diagnostic tool of choice.
Sonographically, under optimal sonic conditions, after fluid filling of the stomach, space-occupying lesions of the gastric wall can be identified. Large and constant cocardia are suspect, and sonographically controlled palpation shows the tumor to be poorly deformable [9].
Computed tomographic examinations are rarely requested primarily for the diagnosis of gastric carcinoma. In staging, the method has proven useful to verify wall-spanning tumor growth, lymph node or organ metastases. In the stomach well-filled with oral water, wall thickenings with more than 4 mm are tumor-suspect, nodular, or irregularly contoured [8].
Magnetic resonance imaging can differentiate four morphologic forms of adenocarcinoma (review 2). The tumors are isointense to the gastric wall in T1w, slightly hyperintense in T2w, and show marked signal enhancement after contrast administration [10].
Case studies
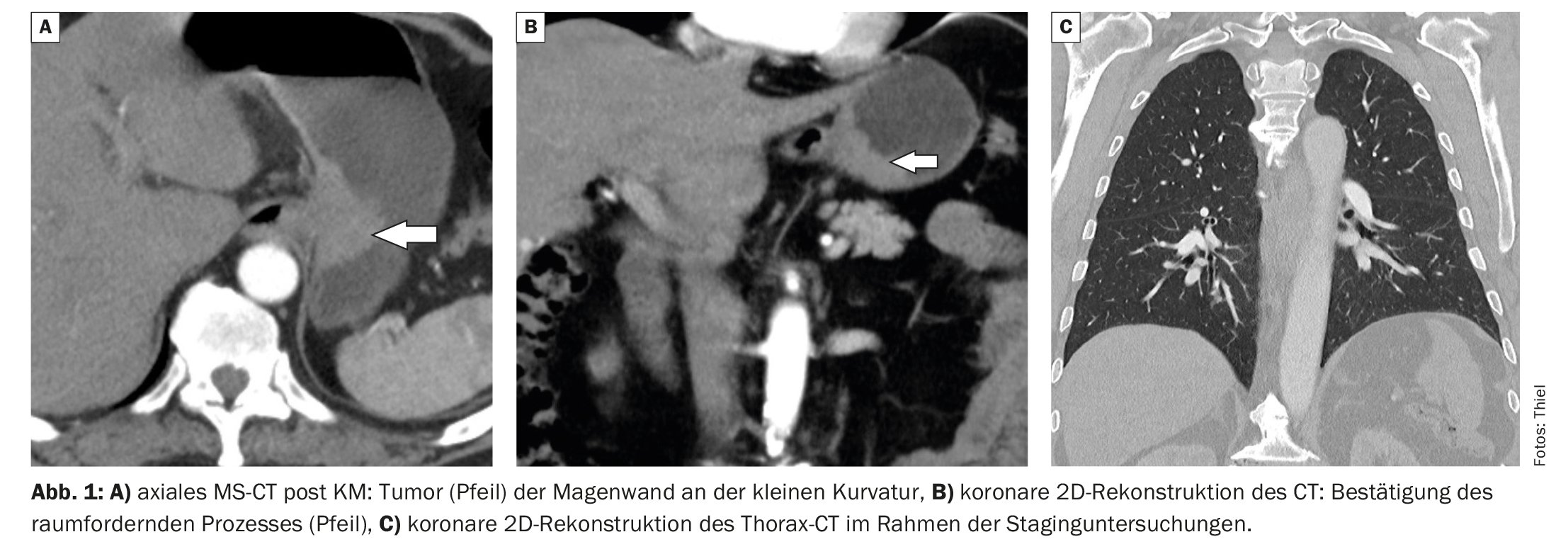
The first case report shows histologically confirmed adenocarcinoma of the stomach in a 72-year-old patient (Fig. 1A and B) with upper abdominal pain, nausea, weight loss, and loss of appetite. Pulmonary filiae were excluded during staging (Fig. 1C).
In case report 2, CT detected gastric carcinoma in the distal corpus and pylorus (Fig. 2A to C). The 51-year-old patient presented with mid-abdominal pain, fatigue, fatigue, and vomiting. Histologically, gastric carcinoma was also confirmed.

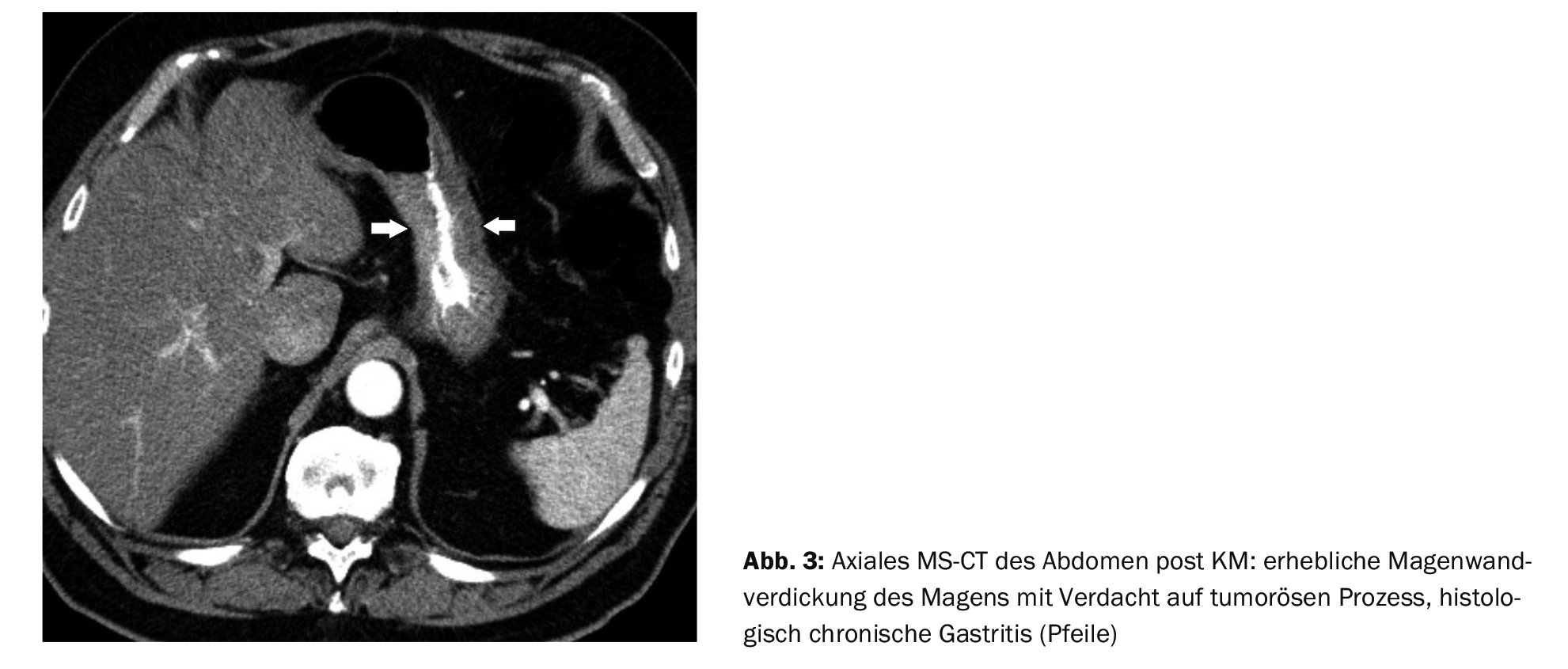
Case report 3 shows that CT has great sensitivity but lower specificity in the diagnosis of gastric mucosal tumors. In the case of the 72-year-old patient with prostate carcinoma, a conspicuous thickening of the gastric wall was also seen during staging (Fig. 3) , but could be histologically assigned to chronic gastritis.
Take-Home Messages
- Adenocarcinoma is the most common malignant tumor of the stomach.
- The incidence has been declining in recent years.
- The malignancy is slightly more common in men than in women,
primarily in the middle stage of life. - The diagnostic method of choice is endoscopy, which also includes a
histological backup is possible. - Cross-sectional imaging techniques are highly valued in staging.
Literature:
- Ajani JA, et al: Gastric adenocarcinoma. Nat Rev Dis Primers 2017; 3: 17036.
- Arfaoui D, et al: Epidemiologic profile of gastric carcinoma: study of 140 cases. Tunis Med 2006; 84(5): 301-304.
- Burgener FA, et al: Differential diagnostics in MRI. Georg Thieme Verlag: Stuttgart, New York, 2002; 555.
- Dietel M, Suttorp N, Zeitz M (eds.): Harrison’s Internal Medicine. Volume 1. 17th edition. ABW Wissenschaftsverlag GmbH: Berlin 2009; 709.
- DocCheck Flexicon, https://flexikon.doccheck.com/de/Perniziöse_
Anemia, (last accessed Dec 14, 2022). - Medicoconsult, www.medicoconsult.de/morbus_menetrier, (last accessed Dec. 141, 2022).
- Prokop M, Galanski M (Eds): Computed Tomography of the Body. Georg Thieme Verlag: Stuttgart, New York 2003; 559-561.
- Rebai W, et al: Early gastric adenocarcinoma. Tunis Med 2010: 88(1): 1-4.
- Stahl M: Gastric cancer – symptoms, www.krebsgesellschaft.de/basis-informationen-krebs-allgemeine-informationen.html,
(last call 12/14/2022) - Struve C: Sonography of the abdomen. 4th, revised and expanded edition. Urban & Schwarzenberg: Munich, Vienna, Baltimore 1991; 87.
FAMILY PRACTICE 2023: 18(1): 40-42









