Why do people lose weight unintentionally? This question was discussed in a workshop at the ESCIM Congress in Geneva. Seniors in particular often come to the family doctor’s office with such symptomatology, without it being addressed in more detail. So some awareness of this issue among primary care providers is needed.
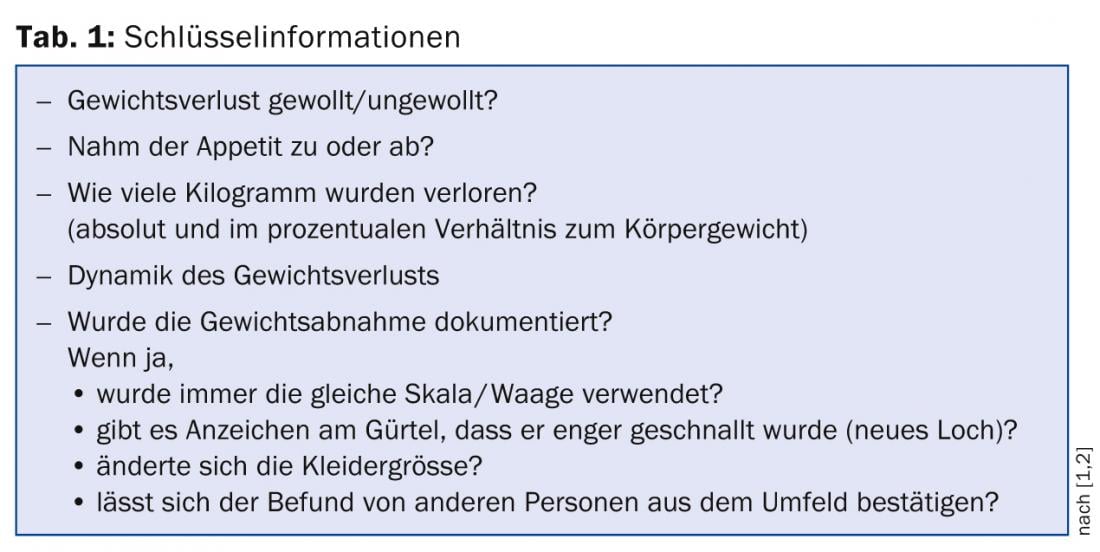
(ag) PD Dr. med. Andreas Zeller, senior physician at the Institute of Family Medicine at the University of Basel, started by going into more detail about the definition of the term: “First, we have to define what unwanted weight loss is in the first place: it is a loss of more than 5% of body weight over six (to twelve) months. However, definitions in the literature are not consistent. Most commonly, it is about 4.5 kg or more that is considered unwanted weight loss over this period. However, there are daily variations in body weight of up to two kilograms,” Dr. Zeller explained. The key information to obtain from the patient is shown in Table 1 .
Additional information can be obtained by systematically querying the following factors:
- Dental Health (Denture?)
- Dysphagia/Odynophagia
- Vomitus
- Diarrhea/Melena
- Abdominal pain
- Digestive/intestinal changes.
“You should also examine the patient for his eating habits, for example, ask him directly what he ate yesterday,” Dr. Zeller said. “Also relevant are signs of polyuria, icterus, HIV risk, alcohol and cigarette use, travel and fever, and psychosocial stress or depression. Most important in diagnosing weight loss remain the patient history and physical examination. They guide the next steps and define the necessary tests. Nonspecific all-around testing yields little gain [3].”

Further procedure
What are the next steps once the initial baseline examinations (clinical picture, standard laboratory tests, chest x-ray, and abdominal ultrasound) are normal? A Belgian study [4] has shown that in this case both severe organ diseases in general and malignant tumors in particular are rare. In the following six months, therefore, a “watchful waiting” strategy can usually be adopted, according to Dr. Zeller.
Reasons for weight loss
A German prospective follow-up study [5] found that no reason for weight loss could be found in about 16% of the 158 elderly participants. What does this mean now? “In any case, one must not fall into the prejudice that weight loss in older people is normal with the aging process. Of course, seniors often lose weight – but age alone does not make you lose weight. You should therefore also look here to see whether there is a detectable reason for this symptom,” Dr. Zeller emphasized. “An important factor that should not be forgotten is malnutrition: older people often find it difficult to go shopping themselves and to get enough and varied food. This problem is encountered primarily by family physicians, since seniors present here more frequently. The likelihood of such individuals needing hospitalization, as well as the risk of infection, poor wound healing, muscle decline and even death, increase if the disorder goes undetected.” 60% of patients in the above study declined due to non-malignant diseases (psychological disorders accounted for 11%). Malignant causes were found mainly in the gastrointestinal area. “Such tumors in the gastrointestinal tract are definitely a common cause of unintentional weight loss,” Dr. Zeller said.
Since depression is also often responsible for weight loss, it should be briefly interrogated in practice, using two factors: Have you experienced the following in the last two weeks?
- Little interest or pleasure in things (anhedonia)
- Low spirits, depressed or hopeless state (mood).
These two screening questions provide a good initial estimate of whether or not depression is present [6].
Search for treatable causes
According to Dr. Zeller, therapy is based on the causes. Mirtazapine (Remeron®), for example, is used to increase appetite and treat depression. Furthermore, lingual tablets before the meal (metoclopramide) or so-called “food additives” can be used.
Source: “Unwanted weight loss: evidence-based approach in practice,” workshop at ESCIM Congress, May 14-16, 2014, Geneva.
Literature:
- Marton KI, Sox HC Jr, Krupp JR: Involuntary weight loss: diagnostic and prognostic significance. Ann Intern Med 1981 Nov; 95(5): 568-574.
- Winfield RA: Letter: Weight loss and the belt. Ann Intern Med 1973 Dec; 79(6): 910.
- Huffman GB: Evaluating and treating unintentional weight loss in the elderly. Am Fam Physician 2002 Feb 15; 65(4): 640-650.
- Metalidis C, et al: Involuntary weight loss. Does a negative baseline evaluation provide adequate reassurance? Eur J Intern Med 2008 Jul; 19(5): 345-349. doi: 10.1016/j.ejim.2007.09.019. epub 2007 Nov 26.
- Lankisch P, et al: Unintentional weight loss: diagnosis and prognosis. The first prospective follow-up study from a secondary referral centre. J Intern Med 2001 Jan; 249(1): 41-46.
- Arroll B, Khin N, Kerse N: Screening for depression in primary care with two verbally asked questions: cross sectional study. BMJ 2003 Nov 15; 327(7424): 1144-1146.
HAUSARZT PRAXIS 2014; 9(7): 42-43