One of the most important decisions that must be made at the beginning of a symptomatic myeloma is the appropriate therapy. While not yet curable, a number of good options exist that can delay progression. Based on intensive research and better understanding of the pathophysiology, effective treatment options could be added to chemotherapy.
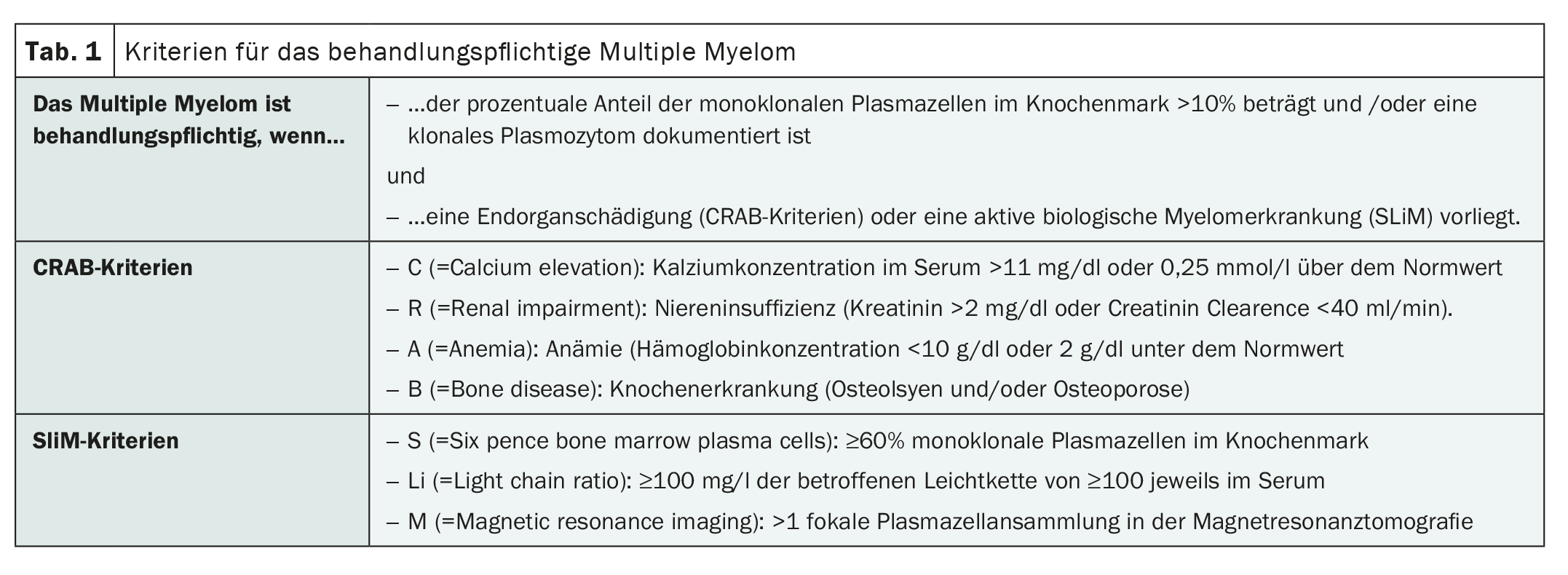
Not every multiple myeloma requires treatment from the outset. If there are no clinical signs yet, the patient can be closely monitored and observed for the time being. However, as soon as bone changes become apparent, for example, effective treatment is indicated. A symptomatic disease is present if, for example, the CRAB criteria are met:
C = increased calcium concentration in the blood (hypercalcemia),
R = Renal dysfunction (renal insufficiency),
A = anemia (anemia),
B = Bone destruction (Table 1) .
The average life expectancy for patients with newly diagnosed multiple myeloma is 5 years. Staging and prognostic classification are essential for deciding on a suitable treatment regimen. The aim is to improve myeloma symptoms, reduce the M protein and control the disease.
Focus on treatment management
The different therapeutic approaches are based on conventional chemotherapy, high-dose chemotherapy with autologous blood stem cell transplantation and newer substances. In order to achieve the greatest possible effect against the tumor cells during chemotherapy and at the same time reduce side effects, combinations of cytostatic drugs with different effects are often used. If possible, however, high-dose chemotherapy with autologous stem cell transplantation should be resorted to. This procedure is currently the standard procedure for patients up to around 70 years of age. In 20-60% of those affected, a complete remission can be achieved in this way, which can last for several years. Success depends not least on the choice of treatment before and after the actual chemotherapy. A combination of the two most important substance classes, proteasome inhibitors and immunomodulators, appears to be promising for this purpose.
Established and effective
Thalidomide, bortezomib and lenalidomide have already proven their worth in the treatment of multiple myeloma in multiple therapy regimens, although thalidomide is now only rarely used. As a proteasome inhibitor, bortezomib has a high response rate in primary and relapse therapy. Among other things, it blocks the activation of certain signaling pathways and DNA repair mechanisms in the myeloma cell so that the cells’ resistance to cytostatic drugs can be overcome. Bortezomib is often used as a triple combination with dexamethasone and cyclophosphamide (VCD), for example. Lenalidomide belongs to the group of immunomodulators. It impairs the release of pro-inflammatory substances and increases the production of anti-inflammatory substances.
Safe treatment for older patients too
For the treatment of older patients >70 years of age or patients with many comorbidities, the only option for a long time was a combination therapy of melphalan and prednisone (MP). A significant improvement in efficacy was then achieved by adding bortezomib. Compared with MP, the MPV combination led to a significant improvement in the prognosis of the affected patients. Current results suggest that an extension of this treatment regimen to include an antibody directed against the CD38 molecule could lead to a further improvement in therapy results. Therapy with CAR-T cells and bispecific, T cell-activating antibodies of various biological forms also has great potential.
Further reading:
- https://multiples-myelom.ch/de/multiples-myelom/therapien (last accessed on 12.04.2024)
- https://lymphome.de/multiples-myelom/therapie (last accessed on 12.04.2024)
- www.krebsgesellschaft.de/onko-internetportal/basis-
informationen-krebs/krebsarten/multiples-myelom-plasmozytom-morbus-kahler/therapie.html (last accessed on 12.04.2024). - www.onkopedia.com/de/onkopedia/guidelines/multiples-myelom/@@guideline/html/index.html (last accessed on 12.04.2024).
InFo ONCOLOGY & HEMATOLOGY 2024; 12(2): 36