
Although the treatment of arterial hypertension is part of the “daily bread” in family practice, it also causes headaches time and again. This is because there are a number of pitfalls on the road to controlled blood pressure that prevent effective blood pressure reduction. An overview of the most common problems and possible solutions was presented at Medidays in Zurich by PD Dr. med. Lukas Zimmerli, ESH Hypertension Specialist and Deputy Chief Physician of the Department of Internal Medicine, University Hospital Zurich.
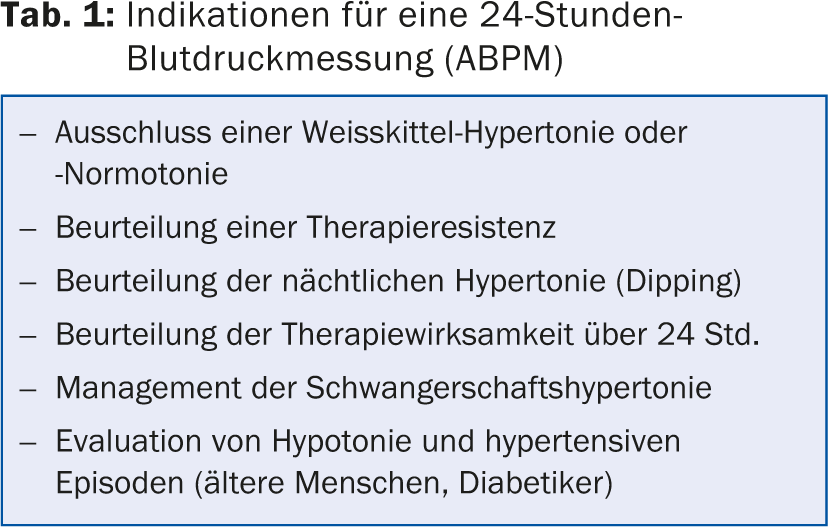
At the beginning of his presentation, Lukas Zimmerli advocated the low-threshold use of 24-hour blood pressure measurement (ABPM), because the mean blood pressure value over 24 hours, or the daytime and nighttime averages correlate significantly better with cardiovascular risk and end-organ damage than individual values measured in practice. ABPM also offers the possibility of detecting white coat hypertension or white coat hypertension. -normotension as well as to clarify resistance to therapy (tab. 1). “However, ABPM is not useful for very high blood pressure values above 180 mmHg,” said the speaker. “It’s painful for these patients to have the blood pressure cuff inflated to 240 mmHg every 20 minutes. In such a situation, hypertension should be treated first, and only then do you do ABPM to monitor therapy.”
Different standard values with different measurement methods
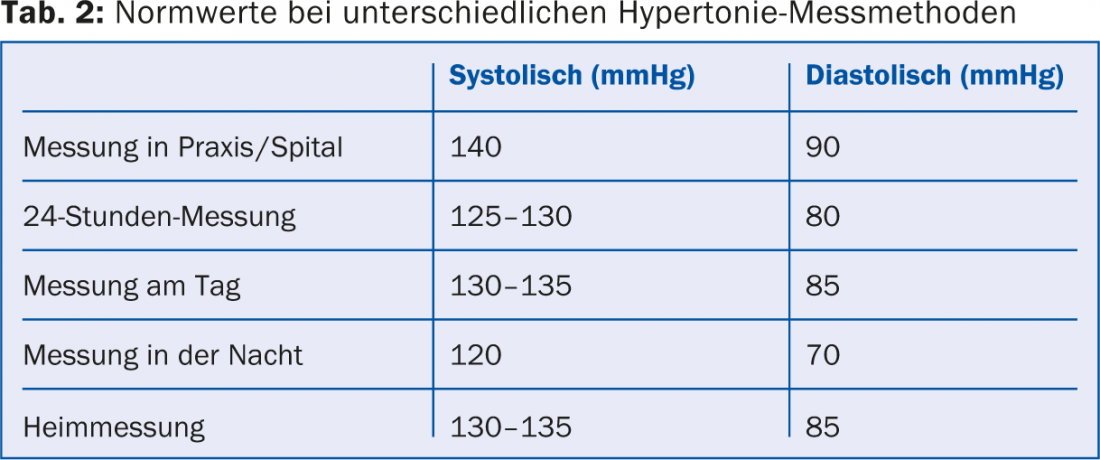
It is important to know the standard values for the various measurement methods and also to explain these to the patient (Tab. 2). Different consequences result from the different values measured:
- Home measurement >135/85 mmHg, office measurement >140/90 mmHg: uncontrolled hypertension.
- Home measurement >135/85 mmHg, office measurement <140/90 mmHg: masked hypertension (about one in eight patients with normal blood pressure values in the office).
- Home measurement <135/85 mmHg, office measurement >140/90 mmHg: white coat hypertension (affects 10-15% of the population).
- Home measurement <135/85 mmHg, office measurement <140/90 mmHg: controlled hypertension or normal blood pressure.
Risk factors for non-conformity of blood pressure values in practice and at home are male gender, obesity, age over 65 years and alcohol consumption.
Rotation through the substance classes
With monotherapy of the first drug used, only 40% of hypertensive patients can be satisfactorily controlled. If monotherapy were rotated through all substance classes, it would be about 75%. It may therefore be worthwhile to be patient when adjusting blood pressure and to switch between different substance classes, especially in patients who suffer from many side effects. In the Swiss guidelines for hypertension therapy (www.swisshypertension.ch), beta-blockers are in a worse position than in the European guidelines, where beta-blockers are placed on an equal footing with the other substance classes.
Secondary hypertension
In the search for a secondary cause of hypertension, one should be guided primarily by the clinic and examination findings – imaging plays only a secondary role. The most common causes of secondary hypertension are renal disease, renal artery stenosis, and primary aldosteronism; rare causes are pheochromocytoma or Cushing’s syndrome.
Hypertensive crisis
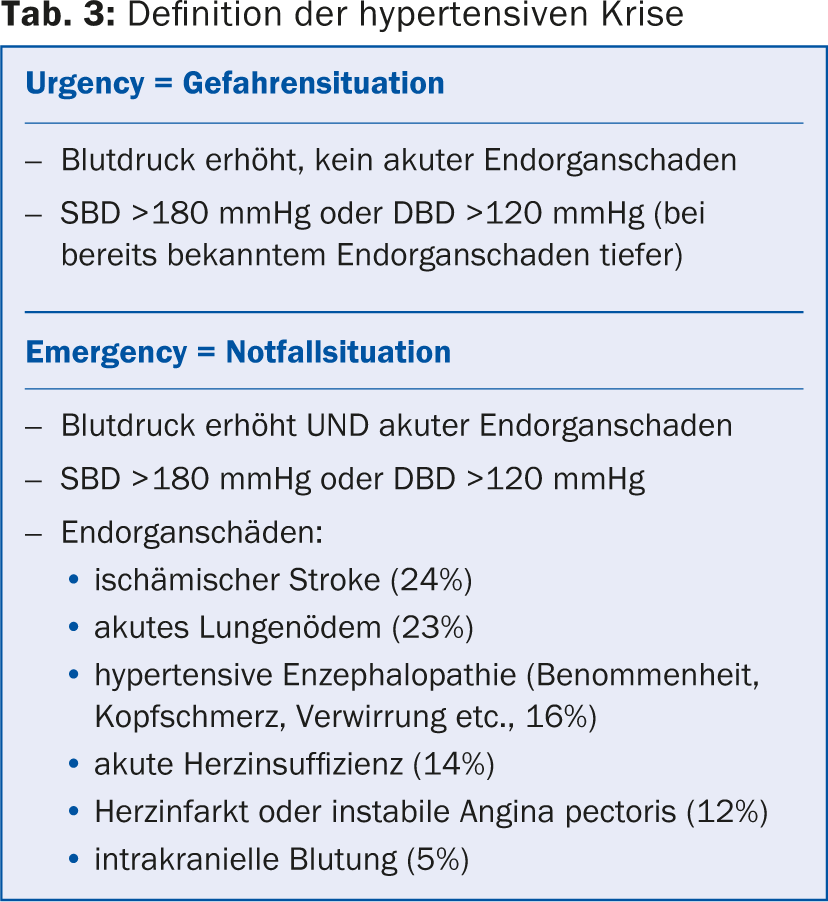
In the case of very high blood pressure values, a distinction is made between a dangerous situation (“Urgency”) and an emergency situation (“Emergency”) (Tab. 3). It is worthwhile to take an exact medical history, incl. Questions about medication compliance and use of hypertensive medications and drugs (cocaine, amphetamines, NSAIDs, chondrosulf, etc.). “In the USZ, most patients with a hypertensive crisis are longtime hypertensives with a medication problem, such as running out of pills,” said PD Lukas Zimmerli, MD.
In a hypertensive emergency, blood pressure should be lowered rapidly, but no more than 20- 30% within two hours – the only exception being the fastest possible pressure measurement in aortic dissection or aneurysm. Intravenous medication with short-acting substances is preferred because of better controllability; invasive monitoring may also be necessary. Blood pressure must be lowered carefully because lowering it into the normal range can cause irreversible organ damage in hypertensive patients.
If there is “only” a hazardous situation, the blood pressure should be lowered within 24-48 hours. Oral medication is usually sufficient, and hospitalization is necessary only in cases of refractory high blood pressure. Ensure that the patient continues antihypertensive therapy correctly.
Hypertension and diabetes
New guidelines for hypertension treatment in diabetic patients have been available since last year. In all patients with diabetes, the target blood pressure is <140/90 mmHg. Lower values may be appropriate if they can be achieved without side effects (such as orthostatic hypotension). In patients with diabetic nephropathy and proteinuria, blood pressure below 130/80 mmHg is recommended. The combination of ACE inhibitor and Ca channel blocker appears to reduce mortality the most, followed by the combination of ACE inhibitor and diuretic. Long-acting preparations are preferable, and patients on combination therapy should take one of the drugs at night. When using ACE inhibitors, ARBs, or diuretics, creatinine and potassium levels must be monitored.
Hypertension resistant to therapy
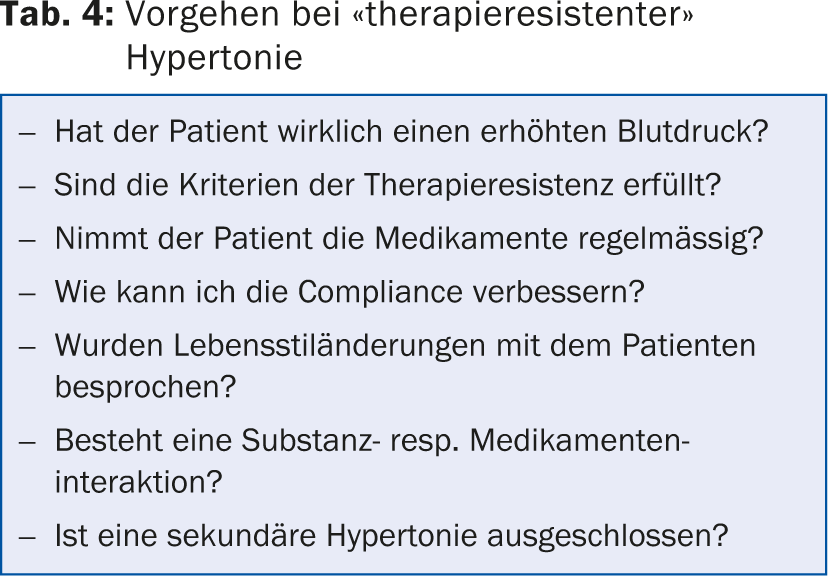
Therapy resistance occurs when target blood pressure values are not achieved despite several weeks of fully exhausted treatment with a three-drug combination including a diuretic. It is advisable to systematically answer some basic questions (Tab. 4). One should not primarily doubt the patient’s compliance, but rather check the substance selection, because the patient may be receiving the wrong substance(s) or drug(s). an insufficient dosage.
However, if compliance is still insufficient, it can often be improved with a single-pill combination. In severe cases, it may be worthwhile to hospitalize the patient: It may be possible to adjust the blood pressure under controlled conditions (supervised medication, no stress from work and family).
Hypertension in old age
15% of the elderly have labile hypertension, that is, a large variability of blood pressure values between measurements. Labile hypertension is an independent risk factor for cardiovascular events. Fitness resp. Frailty plays a major role in elderly patients: fit individuals benefit from blood pressure reduction, whereas frail individuals (in wheelchairs, bedridden) hardly benefit at all.
In general, “start slow, go slow” applies to blood pressure reduction in old age. Low initial doses should be used to minimize side effects, and a slow reduction in blood pressure should be instituted to prevent disturbances in orthostasis. Blood pressure measurement should always be performed in a sitting and standing position. Selection of antihypertensives is usually based on comorbidities.
Hypertension and renal insufficiency
In the presence of microalbuminuria, cardiovascular risk is increased by 50%. It is therefore important to look for and treat albuminuria as a manifestation of end-organ damage, as this will improve outcome. To reduce proteinuria (and blood pressure), salt restriction, , and drug therapy with ACE inhibitors, angiotensin II blockers (ARBs), diltiazem and verapamil, diuretics, and spironolactone, if needed, are suitable. The combination of ACE inhibitors and ARBs is not recommended.
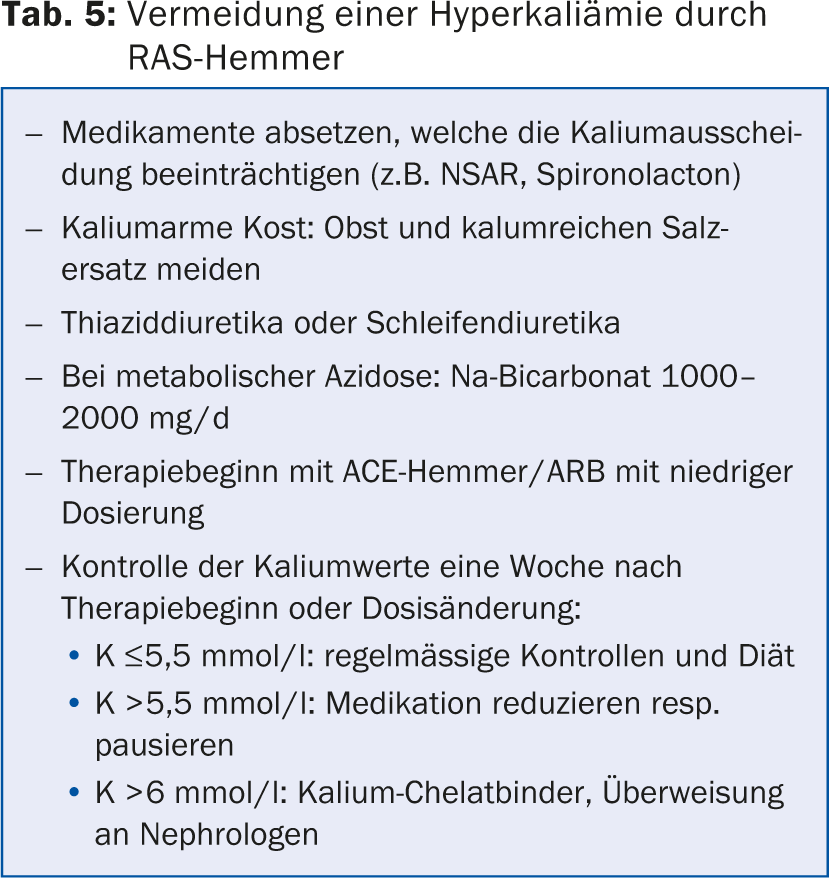
RAS inhibitors carry the risk of hyperkalemia – to avoid this, various measures are appropriate (Tab. 5) . The more severe the albuminuria, the lower the target blood pressure: with albuminuria <30 mg/d, the target blood pressure is ≤140/90 mmHg; with albuminuria from 30 mg/d, the target blood pressure is ≤130/80 mmHg.
Hypertension in pregnancy
If a pregnant woman’s blood pressure readings are too high, the question is whether it is pre-existing hypertension, gestational hypertension, or already preeclampsia. If blood pressure is too high before the 20th week of pregnancy (SSW), there is usually pre-existing hypertension (in 1-5% of all pregnancies). If there is hypertension after the 20th week of gestation and other symptoms such as proteinuria, rising serum urea, liver dysfunction, etc., there is preeclampsia.
In pregnant women, blood pressure should be measured while seated and to the nearest 2 mmHg, using a device validated for pregnant women and an adequate cuff size. A 24-hour ambulatory measurement can help rule out white coat hypertension, which is present in up to one-third of pregnant women with elevated blood pressure, or diagnose nocturnal hypertension, which is associated with a higher risk of maternal and fetal complications. There is only a maternal indication for the therapy of hypertension during pregnancy (prevention of cardiovascular complications), but a positive influence on the child has not yet been demonstrated. Blood pressure therapy also does not reduce the risk of preeclampsia or miscarriage. Blood pressure should not be lowered aggressively to avoid growth restriction of the child; at most, medication is reduced in the second trimester.
Erectile dysfunction
About one-third of all men with hypertension have erectile dysfunction (ED). This can be triggered by the hypertension itself, but also by the therapy. Beta-blockers and diuretics in particular often have a negative impact on erectile function. If possible, patients with ED should have their blood pressure medication switched (to ARBs); if ED persists, a PDE-5 inhibitor may also be given. Men on combination therapies can also take these agents without risk, but caution is advised when taking alpha blockers (PDE-5 inhibitor low dose and swallow delayed with antihypertensive). Absolutely contraindicated is the combination of nitrates and PDE-5 inhibitors.
Conclusion
- Observe different standard values of blood pressure (office measurement, outpatient measurement, 24-hour measurement)
- Rotation through the antihypertensive drug classes may be worthwhile
- Search for secondary hypertension according to clinic
- Hypertensive crisis: differentiation according to “Urgency” and “Emergency
- Diabetes: Target blood pressure <140/90 mmHg
- Therapy resistance: is present with triple therapy incl. Diuretic
- Old patients: “start slow, go slow”.
- Renal insufficiency: look for albuminuria (as a sign of end organ damage).
- Pregnancy: therapy if blood pressure values ≥160/110 mmHg
- Do not forget the sexual anamnesis!
- More detailed information at www.eshonline.org/Guidelines/ArterialHypertension.aspx
Source: Medidays, September 3, 2014, University Hospital Zurich
HAUSARZT PRAXIS 2014; 9(11): 56-60









