Wilms’ tumor is now a prime example of an approximately curable malignant disease. The avoidance of side effects and late effects of treatment is becoming increasingly important in this context.
Wilms’ tumor is an embryonal, malignant, solid tumor of the kidney. It was first classified as a renal neoplasm by Rance in 1814 [1] and described by the surgeon Max Wilms in 1899 in the 90-page monograph “The Mixed Tumors of the Kidney” [2]. Advances in medicine, especially in surgery, radiotherapy, and the development of effective chemotherapies, as well as interdisciplinary collaboration in the context of prospective randomized therapy trials, have turned what was once always a tumor leading to death into a prime example of a curable malignant disease today.
Epidemiology
About 6% of all malignant neoplasms in children and adolescents are Wilms tumors (nephroblastomas). The incidence of Wilms tumor is thus 7 per 1,000,000 children under 15 years of age; it is slightly more common in girls than in boys [3], with an age peak between the second and third years of life.
Etiology
Causes for the development of nephroblastoma are largely unknown. However, Wilms’ tumor occurs more frequently in association with syndromes. These include WAGR syndrome, Denys-Drash syndrome, Beckwith-Wiedemann syndrome, and Perlman syndrome, as well as Recklinghausen neurofibromatosis. Two Wilms tumor genes play a role in syndrome-associated nephroblastomas: the wt1 gene on chromosome 11p13 and the wt2 gene on chromosome 11p15.5. In addition, nephroblastoma also occurs associated with other abnormalities.
Genetics
Nephroblastoma is a genetically heterogeneous tumor. Mechanisms of tumor development are gene mutations, loss of heterozygosity (LOH) and loss of imprinting (LOI). Several genes play a critical role in the development of nephroblastoma. However, to date, only the Wilms tumor suppressor gene wt1 has been cloned on chromosome 11p13 [4]. Deletions of this gene are found in 10-30% of nephroblastomas [5]. LOH most commonly (approximately 40%) affects 11p [6]. There is evidence that, in addition to the wt1 gene mentioned above, a second gene in 11p15.5, the wt2 gene, may have a role in the development of nephroblastoma. LOH is also found from chromosome 16q, which is the case in about 20% of tumors. It is concluded that there is a third Wilms tumor gene, the wt3 gene [7,8]. Molecular biology-oriented research is currently attempting to identify prognostically significant gene combinations with the aid of gene chip arrays or gene expression analyses [9,10].
A familial accumulation in the occurrence of a Wilms tumor is present in about 1% of all children. It follows an autosomal dominant mode of inheritance with variable penetrance [11]. This includes all bilateral tumors. Most unilateral tumors are not hereditary.
Nephroblastomatosis
Nephrogenic remnants or nephroblastomatosis may occur and be diagnosed as a precursor of nephroblastoma [12]. The definition of nephroblastomatosis is constantly changing. This should include all lesions that are potential precursors of nephroblastoma. Nephroblastomatosis is then defined as the diffuse or multifocal appearance of nephrogenic remnants. Nephroblastomatosis shows hallmarks of potentially malignant degeneration to nephroblastoma.
Histopathology
According to the theory of Max Wilms, nephroblastoma is a tumor of mesodermal origin and arises in the embryonic kidney. As a result, there is a variety of differentiations. The classic Wilms tumor of the so-called mixed type is a renal tumor with a blastemic, epithelial (tubules) and mesenchymal component (stroma). The proportion of these three components may vary, so that one cannot always speak of a triphasic tumor. The ultimate diagnosis of a Wilms tumor is still based on the histopathologic classification [13]. Most often, Wilms tumor occurs on one side. But bilateral tumors occur in about 5-7% of cases. Macroscopically, Wilms’ tumor presents as a solid mass that can cross the kidney. It is often lobulated, but may also have cystic portions.
Classification
According to the different approaches of the two therapy optimization studies of SIOP (Société Internationale d’Oncologie Pédiatrique) and NWTS (National Wilms Tumor Study Group), respectively, Wilms tumors are classified histopathologically. The difference between the two classifications is based on the different therapeutic approach. In SIOP, tumor histology is performed only after preoperative chemotherapy; in NWTS, classification is performed after primary resection (tumor nephrectomy). For primary chemotherapy-pretreated patients, this is done according to SIOP using a version of the 1995 Stockholm-Working classification revised in 2002 (Table 1) [14].

If patients underwent primary tumor nephrectomy, they are classified as low, intermediate, or high malignancy, or as favorable (“favorable”) or unfavorable (“unfavorable”) histology according to the NWTS classification. Evidence of anaplasia is of prognostic significance beyond stage I [15].
Staging and prognosis
In addition to histologic subtyping, prognosis in Wilms tumor depends on tumor stage. Staging requires an accurate description of the intraoperative extent of the tumor, which is supplemented by histologic examination. According to the SIOP criteria, this is done after preoperative chemotherapy. The specific determination of tumor stage is of considerable clinical importance for subsequent risk stratification and therapy. The local (abdominal) stage of the primary tumor should always be indicated. The staging according to SIOP, which is essentially the same as NWTS, is shown in Table 2.
The prognosis of nephroblastoma remains dependent on the response to preoperative chemotherapy [16]. Here, both tumor volume and histopathologic subtype are assessed after previous chemotherapy [16]. Furthermore, several genetic markers (LOH of 11q, 16q, 22q and p53 mutations) seem to correlate with an unfavorable prognosis [17]. Specific tumor markers do not exist in Wilms’ tumor.

Today, 90% of all children with a Wilms tumor can be cured. In this context, patients with low and intermediate malignancy with non-metastatic tumor have a survival prognosis of more than 90%. In contrast, patients with diffuse anaplasia or a blast-rich subtype have a much less favorable prognosis [15,16]. If distant metastases are present, the prognosis of patients is critically dependent on the response to the chemotherapy performed. If remission can be achieved after preoperative chemotherapy and complete tumor resection, patients have a survival rate of 80% [16,18].
Clinic and symptomatology
The leading symptom of Wilms’ tumor is typically a painless, palpable, or even visible abdominal tumor. Patients are usually asymptomatic, and abdominal pain or macrohematuria are rare. Cough may be a clinical symptom of pulmonary metastasis. Very rarely, hypertension or coagulation disorders occur.
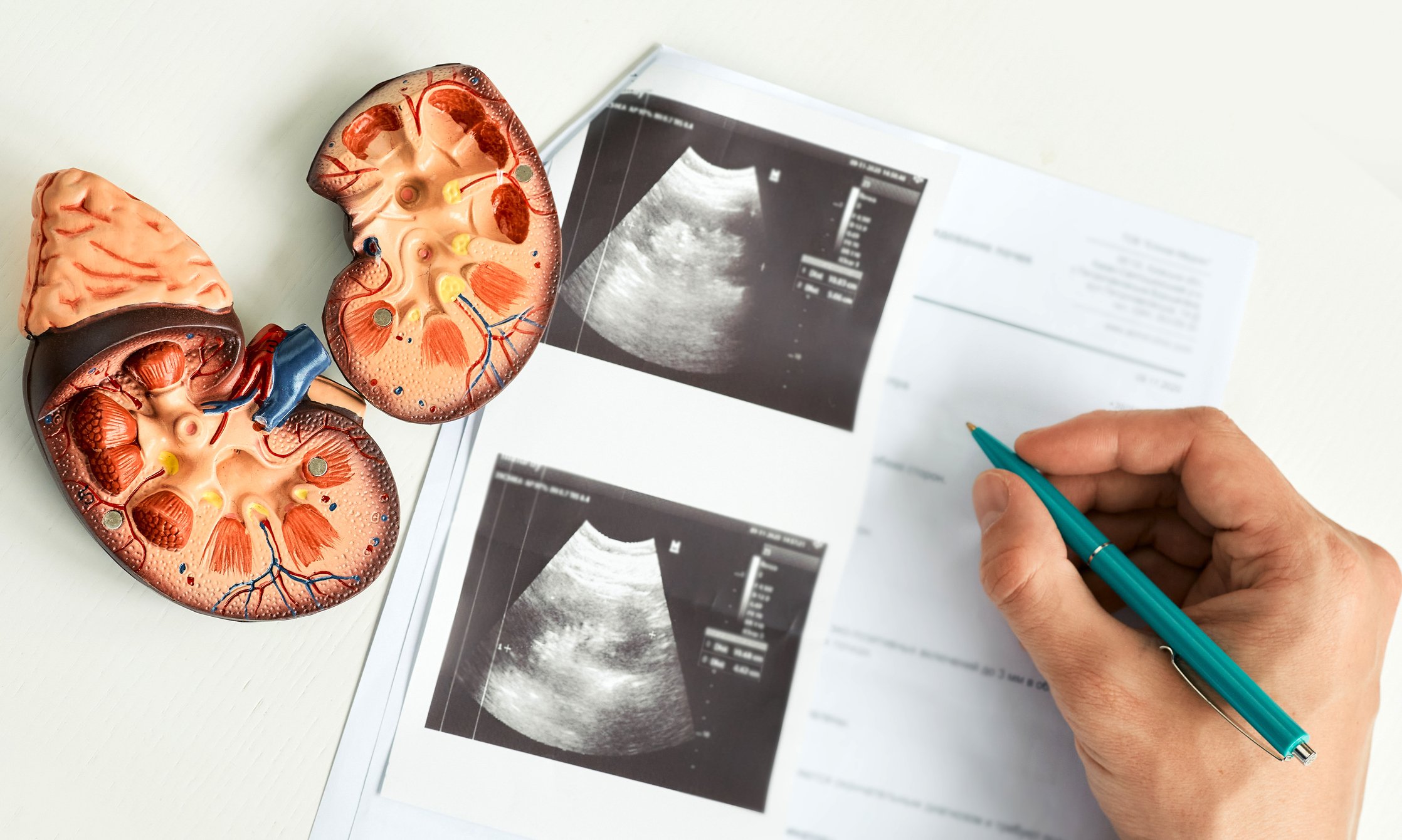
Imaging
According to the SIOP, imaging techniques are used to confirm the primary diagnosis [19,20]. This includes sonography as well as a sectional imaging procedure such as computed tomography (CT) or magnetic resonance imaging (MRI). These are each performed natively and with contrast agent administration. Possibly, these procedures are supplemented by excretion urography. Characteristic findings that usually allow the diagnosis to be made are shown in Overview 1 [20]. Naturally, there is some risk of misdiagnosis when imaging alone is used to make the diagnosis. This may lead to patients who have not had histopathologic confirmation of the diagnosis of nephroblastoma to receive preoperative chemotherapy.

Differential diagnosis
Differential diagnoses of nephroblastoma include neuroblastoma, renal cell carcinoma, rhabdoid tumor, nephroblastomatosis, teratoma, ganglioneuroma, cystic nephroma, hamartoma, renal cysts, adenoma, hematoma, renal abscess, lymphoma of the kidney, xanthogranulomatous pyelonephritis, angiomyolipoma, and others.
Therapy Optimization Studies
The 5-year survival rate of patients with nephroblastoma exceeds 90% [16]. This cure rate is due to the prospective studies of SIOP and NWTS, which have translated knowledge gained since 1969 (NWTS) and 1979 (SIOP) into appropriate treatment protocols. These form the basis of today’s therapy optimization studies. Further improvement of therapy, reduction of side effects and late effects of the disease, better risk stratification and finally further improvement of the prognosis of nephroblastoma are the task and goal of these therapy optimization studies. Therefore, the treatment of children with Wilms’ tumor makes sense only according to the appropriate treatment protocols. In the various studies, the three basic pillars of therapy – surgery, chemotherapy and radiation – are applied to varying degrees. The significant reduction in intraoperative tumor rupture and the marked increase in the number of patients presenting with local stage I after surgery argue for the use of preoperative chemotherapy. This can reduce postoperative therapy, especially radiation.
For children and adolescents with a malignant kidney tumor, SIOP 2001/GPOH represents the last current therapy optimization study for all patients in Germany, Austria and Switzerland. It is the continuation of the SIOP 93-01 study, which was valid until June 2001 [21]. The future study will be SIOP UMBRELLA 2016, which is SIOP’s eighth therapy optimization study under a newly created SIOP-Renal Tumor Study Group (RTSG) structure [22].
Wilms tumor therapy
Chemotherapy: The basis for the therapy concept of SIOP is the combination of polychemotherapy with local surgical and radiotherapeutic treatment. Nephroblastoma usually responds well to treatment with cytostatics, so this is an essential part of the treatment regimen. In this context, the treatment of Wilms’ tumor is neoadjuvant. It begins with chemotherapy to reduce the size and partially devitalize the tumor. This is followed by definitive local treatment by surgery, tumor nephrectomy. Further treatment is carried out according to the results of the histological examination of the tumor and the post-surgical stage. This again provides for polychemotherapy and, if necessary, radiation. Preoperative chemotherapy is generally administered to all patients older than six months and younger than 16 years of age if the imaging diagnosis is certain. As stated above, this can achieve a reduction in tumor volume, increasing the proportion of patients with local stage I to 60%. In addition, the rate of surgically induced tumor rupture was reduced to less than 5%. In patients with a bilateral tumor, preoperative chemotherapy is individualized. The goal here is in any case to be able to perform a tumor resection that preserves the kidney. An exception to preoperative chemotherapy is infants less than six months of age who undergo primary surgery, as other tumors are common at this age, such as congenital mesoblastic nephroma.
Postoperative therapy depends on the surgical stage and histologic subtype. Tumors with low malignancy (favorable histology) are usually stage I, and patients with disease age less than six months do not receive preoperative chemotherapy. Because the prognostic advantage of postoperative chemotherapy has not been proven for complete tumor removal, treatment is stopped after surgery. In children with residual tumor postoperatively (stage III), treatment is according to the criteria for intermediate malignancy (standard histology). Approximately 45% of patients with Wilms tumor present with stage I nephroblastoma with intermediate malignancy (standard histology). If stage II or III is present, patients are randomized to receive either two- or three-drug therapy for 28 weeks.
In patients with initial stage IV, a distinction is made between the group of so-called responders, in whom metastases are no longer detectable after six weeks of preoperative chemotherapy, and the group of non-responders, in whom metastases are still detectable after six weeks of preoperative chemotherapy. Responders are treated according to histology and stage postoperatively. Radiation of lung metastases is not performed. Postoperative chemotherapy is intensified in non-responders. In any case, complete removal of the metastases should be performed. If remission cannot be achieved, radiation therapy becomes necessary.
Patients with high malignancy (unfavorable histology) are treated according to HIGH RISK as in the treatment of recurrences and non-responders. The value of high-dose chemotherapy with autologous stem cell transplantation (ABMT) in the treatment of high-risk patients with Wilms’ tumor is still unclear and therefore it cannot be generally recommended. However, ABMT is available as a treatment option.
Surgery: tumor nephrectomy serves two purposes. The Wilms tumor must be radically removed, i.e., R0 resection is the goal. In addition, it is important to determine intraoperatively the tumor spread, i.e. the stage. It should be noted that with good quality preoperative imaging, bilateral renal tumor is diagnosed with a high degree of certainty. Therefore, if the contralateral kidney is unremarkable on imaging, exposure of this kidney may not be necessary during surgery [23,24]. If there is intraoperative doubt about the diagnosis of nephroblastoma, biopsy or puncture of the tumor should be considered only if the tumor is considered unresectable, otherwise there is obligatory stage III. The operation is elective. According to the SIOP treatment criteria, local and remote surgical resection of the primary tumor and any metastases are performed after preoperative chemotherapy. Inspection of the abdominal cavity prior to tumor resection is mandatory [25]. If additional tumor lesions are found, e.g. in the liver, diaphragm, lymph nodes, peritoneum, etc., these must also be completely R0-resected.
The principles of tumor nephrectomy were established in the 1950s at Children’s Hospital of Harvard Medical School in Boston [26] by William Ladd and others and are still valid today. They provide for transabdominal access, careful exposure of the affected kidney with absolute avoidance of tumor rupture, transection of the renal vessels, and placement of the ureter as close to the bladder as possible. Locoregional lymph node dissection, or “lymph node sampling,” is essential [27,28]. It is essential for determining tumor stage and thus is a component of risk stratification, postoperative therapy, and prognosis of the patient. Newer surgical therapy concepts include in particular the aspect of renal preserving tumor resection. The arguments for this are motivated by the risk of the presence of bilateral metachronous nephroblastomas, subsequent renal hypertension, contralateral organ loss from trauma, and renal function impairment from intensive chemotherapy. However, these must be critically weighed against the oncologic criteria of radicality. Therefore, the RTSG surgical panel has developed a classification for kidney-preserving tumor resections as part of the future SIOP UMBRELLA 2016 study [29].
Another consideration in Wilms tumor surgery is the increasing importance of minimally invasive, laparoscopic tumor resection. There are now data on this [30,31], but clear guidelines and prospective studies are needed in the future to define the value of the minimally invasive procedure.
Vascular thrombosis in Wilms’ tumor is well known. Vascular tumor extensions into the vena cava, extending subdiaphragmally or beyond into the right atrium, present a special surgical challenge [32]. In any case, these should be operated on after preoperative chemotherapy, because primary surgery of these tumor thrombi was associated with higher morbidity, especially in the NWTS studies [33,34]. Cytostatic pretreatment in this setting can achieve a significant reduction in the size and extent of the tumor thrombus, thereby greatly facilitating resection [35]. A thrombus extending supradiaphragmally or atrially should be operated on under extracorporeal bypass with heart-lung machine, preferably under “low-flow” conditions or even in cardiac arrest, in hypothermia [36]. Relevant surgical complications have been described, and treatment outcomes with a 5-year survival of 74-87% are acceptable, although less favorable than in the overall population [29].
Radiotherapy: Wilms’ tumor is a highly radiosensitive tumor. With the progressive development of SIOP treatment protocols and the knowledge gained therefrom, especially the development of effective chemotherapy combinations, the indication for radiation could be made increasingly restrictive. Currently, the option of radiotherapy is limited to local risk situations and in a few cases to the treatment of lung metastases and liver metastases [15].
In both SIOP and the Children’s Oncology Group (COG), which has taken over the NWTSG’s role in continuing clinical trials, further risk stratification is an important current study goal to avoid, among other things, unnecessary radiation and its late effects and complications.
Unsolved problems and “future directions
The prognosis of children with Wilms tumor is very favorable. Overall survival with unilateral tumor without metastases is 98%, and recurrence-free survival is 88% [37]. Further intensification of treatment does not bring further improvement for the majority of patients [37]. This contrasts with a minority of patients who have a significantly worse prognosis. Factors that condition them are: Anaplasia [38], bladder-rich tumor after chemotherapy, tumor rupture/local stage III [39], primary metastases/stage IV, outside the lung [40–42], early relapse [39,41], combined local and distant recurrence (especially in the liver). [39–41,43,44], LOH [7], telomerase RNA expression. [45] as well as rhabdoid tumor (RTK) and clear cell sarcoma (CCSK) as separate entities.
Another unsatisfactory aspect of Wilms tumor therapy is toxicity and late effects of treatment. Therefore, the most important goal of current therapy optimization studies is to stratify patients according to their risk profile and to treat them in a differentiated manner. Avoiding unnecessary treatments, especially radiation, is also part of this. This particularly affects children under one year of age and those patients with a tumor with low malignancy (“low risk”).
Future approaches to optimize treatment of Wilms tumor include improvement of surgical lymph node sampling or thoracoscopic resection of pulmonary metastases in selected patients.
A very important focus of research is tumor biology, which is of increasing importance with regard to risk stratification.
The use of new therapeutics, e.g. the combination of vincristine and irinotecan [46], or the risk stratification according to unfavorable biological and genetic factors and the adapted therapy [47] will also have an influence on future therapy protocols and, in the best case, on the survival of the affected children [48].
Take-Home Messages
- The prognosis of children with Wilms tumor is very favorable.
- Wilms’ tumor is now a prime example of an approximately curable malignant disease.
- With complete tumor resection, surgery has a key position within a multimodal therapy concept.
- Kidney-preserving tumor removal has an important role today, especially in the treatment of bilateral nephroblastoma.
- In the future, minimally invasive surgery for tumor resection will become important.
- Children with tumor recurrence still have an unfavorable prognosis.
- Future focus will be on risk stratification according to tumor biology and genetics, as well as on the development of even better adapted therapy concepts.
- The avoidance of side effects and late effects of the treatment is of particular importance.
Literature:
- Rance TF: Case of fungus haematodes of the kidneys. Med Phys 1814; 32: 19.
- Wilms M: The mixed tumors of the kidney. Arthur Georgi, Leipzig 1899: 1-90.
- Pastore G, et al: Malignant renal tumours incidence and survival in European children (1978-1997): report from the Automated Childhood Cancer Information System project. Eur J Cancer 2006; 42: 2103-2114.
- Gessler M, König A, Bruns GAP: The genomic organization and expression of the WT1 gene. Genomics 1992; 12: 807-813.
- Grundy P, et al: Familial predisposition to Wilms tumour does not map to the short arm of chromosome 11. Nature 1988; 336: 374-376.
- Grundy P, Coppes MJ, Haber D: Molecular genetics of Wilms tumor. Hematol Oncol Clin N Am 1995; 9: 1201-1215.
- Grundy PE, et al; National Wilms Tumor Study Group: Loss of heterozygosity for chromosomes 1p and 16q is an adverse prognostic factor in favorable-histology Wilms tumor: a report from the National Wilms Tumor Study Group. J Clin Oncol 2005; 23: 7312-7321.
- Maw MA, et al: A third Wilms’ tumor locus on chromosome 16q. Cancer Res 1992; 52: 3094-3098.
- Yuan E, et al: Genomic profiling maps loss of heterozygosity and defines the timing and stage dependence of epigenetic and genetic events in Wilms’ tumors. Mol Cancer Res 2005; 3: 493-502.
- Zirn B, et al: Expression profiling of Wilms tumors reveals new candidate genes for different clinical parameters. Int J Cancer 2006; 118: 1954-1962.
- Ruteshouser EC, Huff V: Familial Wilms tumor. Am J Med Genet C Semin Med Genet 2004; 129: 29-34.
- Beckwith JB, Kiviat NB, Bonadio JF: Nephrogenic rests, nephroblastomatosis, and the pathogenesis of Wilms’ tumor. Pediatr Pathol 1990; 10: 1-36.
- Schmidt D, Beckwith JB: Histopathology of childhood renal tumors. Hematol Oncol Clin N Am 1995; 9: 1179-1200.
- Vujanic GM, et al: Revised International Society of Paediatric Oncology (SIOP) working classification of renal tumors of childhood. Med Pediatr Oncol 2002; 38: 79-82.
- Graf N, Weirich A: Wilms’ tumour – the state of the art. Oncol 1996; 19: 36-42.
- Graf N, Tournade MF, de Kraker J: The role of preoperative chemotherapy in the management of Wilms’ tumor – The SIOP Studies. Urol Clin North Am 2000; 27: 443-454.
- Grundy PE, et al: Loss of heterozygosity for chromosomes 16q and 1p in Wilms’ tumors predicts an adverse outcome. Cancer Res 1994; 54: 2331-2333.
- de Kraker J, et al: Wilms’ tumor with pulmonary metastases at diagnosis: the significance of primary chemotherapy. J Clin Oncol 1990; 18: 1187-1190.
- Babyn P, et al: Imaging patients with Wilms’ tumor. Hematol Oncol Clin N Am 1995; 9: 1217-1252.
- Schenk JP, et al: Pediatric renal tumors – relevance of imaging. Radiologist 2005; 45: 1112-1123.
- SIOP/GPOH (Society for Pediatric Oncology and Hematology): SIOP 2001/GPOH: Therapy Optimization Study for the Treatment of Children and Adolescents with Nephroblastoma. 2003.
- Vujanic G, et al: The UMBRELLA SIOP-RTSG 2016 study pathology and molecular biology protocol. Nature Reviews Urology 2018; 15(11): 693-701.
- Ritchey ML, Coppes MJ: The management of synchronous bilateral Wilms tumor. Hematol Oncol Clin N Am 1995; 9: 1303-1315.
- Ritchey ML, et al: Fate of bilateral renal lesions missed on preoperative imaging: a report from the National Wilms Tumor Study Group. J Urol 2005; 174: 1519-1521.
- Ehrlich PF: Wilms tumor: progress and considerations for the surgeon. Surg Oncol 2007; 16: 157-171.
- Gross RE: Embryoma of the Kidney (Wilms’ tumor) in: The Surgery of Infancy and Childhood. W.B. Saunders, Philadelphia & London 1953; 588-605.
- Shamberger RC, et al: Surgery-related factors and local recurrence of Wilms tumor in National Wilms Tumor Study 4. Ann Surg 1999; 229: 292-297.
- Fuchs J, et al: Surgical aspects in the treatment of patients with unilateral wilms tumor: a report from the SIOP 93-01/German Society of Pediatric Oncology and Hematology. Ann Surg 2009; 249: 666-671.
- Fuchs, J: Current surgical treatment concepts in Wilms tumor. The Urologist 2015; 12: 1784-1791.
- Warmann SW, et al: Minimally invasive nephrectomy for Wilms tumors in children – data from SIOP 2001. J Pediatr Surg 2014; 49(11): 1544-1548.
- Flores P, et al: Laparoscopic total nephrectomy for Wilms tumor: Towards new standards of care. J Ped Urol 2018. pii: S1477-5131.
- Shamberger RC, et al: Intravascular extension of Wilms tumor. Ann Surg 2001; 234: 116-121.
- Ritchey ML, et al: Preoperative therapy for intracaval and atrial extension of Wilms tumor. Cancer 1993; 71: 4104-4110.
- Ritchey ML, et al: Management and outcome of inoperable Wilms tumor. A report of National Wilms Tumor Study-3. Ann Surg 1994; 220: 683-690.
- Szavay P, et al: Surgery of Cavoatrial Tumor Thrombus in Nephroblastoma – A Report of the SIOP/GPOH Study. Pediatr Blood Canc 2004; 43: 40-45.
- Kirschner HJ, et al: Resection of Wilms’ tumor with cavoatrial tumor thrombus under extracorporeal bypass with deep hypothermia. Med Pediatr Oncol 2003; 41: 397-398.
- Reinhard H, Furtwängler R, Graf N. Wilms’ tumor – update 2007. Urologist A 2007; 46: 143-145.
- Dome JS, et al: Treatment of anaplastic histology Wilms’ tumor: results from the fifth National Wilms’ Tumor Study. J Clin Oncol 2006; 24: 2352-2358.
- Reinhard H, et al: Outcome of relapses of nephroblastoma in patients registered in the SIOP/GPOH trials and studies. Oncol Rep 2008; 20: 463-467.
- Breslow NE, et al: Clinicopathologic features and prognosis for Wilms’ tumor patients with metastases at diagnosis. Cancer 1986; 58: 2501-2511.
- Godzinski J, et al: Local treatment for extra-pulmonary metastases in the SIOP-9 initial stage IV Wilms’ tumor patients. Med Pediatr Oncol 2001; 4: 338.
- Varan A, et al: Prognostic significance of metastatic site at diagnosis in Wilms’ tumor. J Pediatr Hematol Oncol 2005; 27: 188-191.
- Szavay P, et al: Primary Hepatic Metastases in Nephroblastoma – A Report of the SIOP/GPOH Study. J Pediatr Surg 2006; 41: 168-172.
- Fuchs J, et al: Surgical Implications for Liver Metastases in Nephroblastoma – Data from the SIOP/GPOH Study. Surg Oncol 2008; 17: 33-40.
- Dome JS, et al: High telomerase RNA expression level is an adverse prognostic factor for favorable-histology Wilms’ tumor. J Clin Oncol 2005; 23: 9138-9145.
- Geller JI: Current standards of care and future directions for “high-risk” pediatric renal tumors: Anaplastic Wilms tumor and Rhabdoid tumor. Urol Oncol 2016; 34(1): 50-56.
- Dix DB, et al: Treatment of Stage IV Favorable Histology Wilms Tumor With Lung Metastases: A Report From the Children’s Oncology Group AREN0533 Study. J Clin Oncol 2018; 36(16): 1564-1570.
- Aldrink JH, et al: Summary article: Update on Wilms tumor. J Pediatr Surg 2018. pii: S0022-3468.
InFo ONCOLOGY & HEMATOLOGY 2018; 6(6): 13-17.