
Calcinosis cutis is a challenging, disabling condition commonly seen in patients with systemic sclerosis or dermatomyositis. Calcinosis cutis in patients with Sjögren’s syndrome is very rare and only a few cases have been documented in the literature. American physicians have now described the case of a patient with a known Sjögren’s diagnosis who presented with calcinosis cutis of the fingers.
The 56-year-old woman with a history of Sjögren’s syndrome, hypothyroidism and hyperlipidemia presented to Dr. Arya P.V. Akhila’s team in the Rheumatology Clinic at Yale New Haven Health/Bridgeport Hospital for follow-up [1]. The diagnosis of Sjögren’s syndrome was made 20 years earlier based on oral and ocular sicca symptoms, strongly positive anti-Ro antibodies and a positive Schirmer test result. Her disease course was characterized by an asymptomatic elevation of creatinine kinase with negative findings of myositis and muscular dystrophy, negative muscle biopsy results and chronic stable autoimmune thrombocytopenia. She had previously taken methotrexate (whose efficacy waned) and low-dose steroids, which were successfully discontinued. Her condition was well controlled with 200 mg hydroxychloroquine daily. She was not taking calcium or vitamin D supplements and her vital signs were in the normal range.
Tretinoin and sodium thiosulfate did not have the desired effect
Her only symptom during hospitalization was small, painless, pinhead-sized yellowish-white nodules at the subcutaneous level of the right fifth finger. She had similar symptoms on the fourth and fifth right fingers, which did not improve with topical tretinoin and intradermal sodium thiosulfate injections and ultimately required surgical resection. The joints were fully mobile with no erythema, swelling or tenderness. Other physical examination findings were normal.
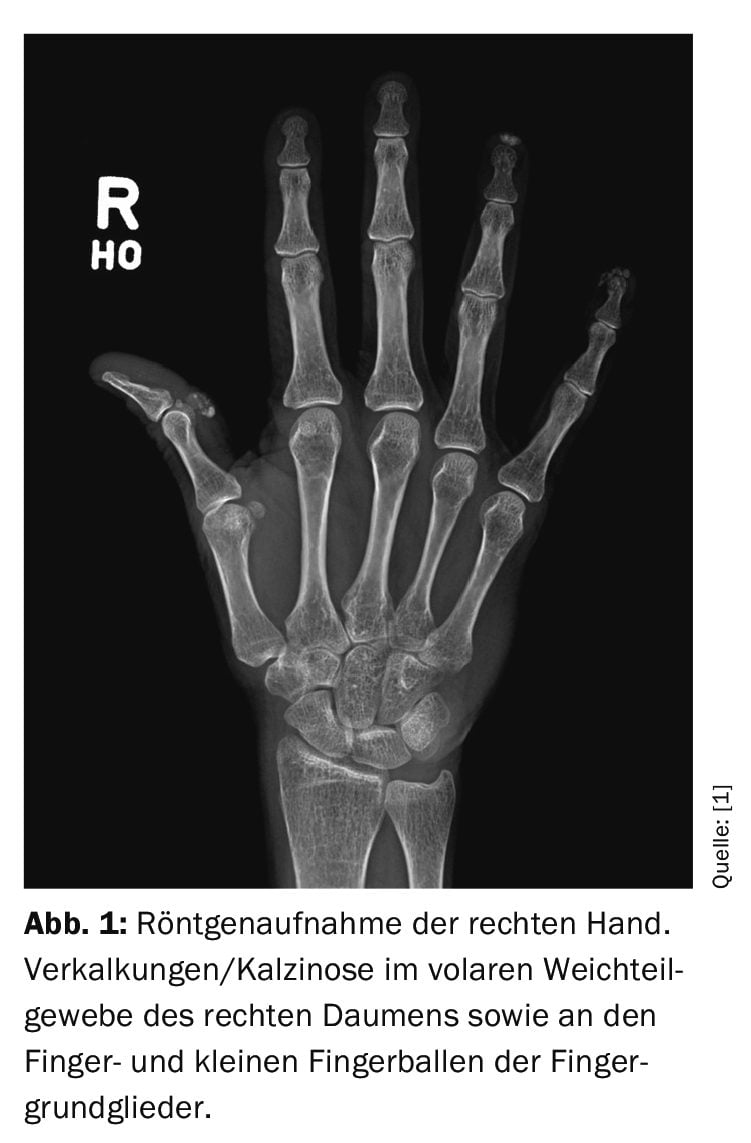
X-ray of the right hand showed soft tissue calcifications in the first and fifth fingers (Fig. 1). Previous skin biopsies showed no signs of scleroderma, but biopsy findings of digital lesions on the right thumb and fourth finger in the past were consistent with calcinosis. As per the patient’s request, she was referred to a dermatologist for surgical curettage of the calcinosis on the fingers. As the disease activity was under control and the inflammatory markers were normal, the treatment of the underlying Sjögren’s syndrome was not changed.
Since calcinosis cutis is rare in Sjögren’s syndrome and the patient had a history of Raynaud’s phenomenon, she was monitored for other clinical or serologic signs of systemic sclerosis or CREST syndrome (esophageal dysfunction, sclerodactyly, telangiectasia).
Patterns and progression are still poorly understood
Calcinosis cutis refers to the accumulation of insoluble calcium salts in the skin and subcutaneous tissue. Depending on the cause, it can be dystrophic, metastatic, iatrogenic, idiopathic or associated with calciphylaxis. Dystrophic calcification often occurs in some autoimmune and inflammatory diseases such as systemic sclerosis and dermatomyositis. However, it is extremely rare in Sjögren’s syndrome, so the predisposing factors, pattern and progression are poorly understood, the authors write. The prevalence of calcinosis varies in different autoimmune diseases. It ranges from 18-49% in systemic sclerosis, 40% in systemic lupus erythematosus and 40-70% in juvenile dermatomyositis compared to 20% in adult-onset cases. It is rarely reported in undifferentiated connective tissue diseases, rheumatoid arthritis and Still’s disease in adults.
The clinical presentation of calcinosis cutis varies, as the authors emphasize. Some patients present with asymptomatic nodules, while others suffer from pain, ulceration and infection. Larger lesions can lead to joint contractures, muscle atrophy and nerve compression due to the mass effect. They can be cosmetically disturbing if they are visible on the skin surface. Previous literature has mentioned a predilection of the upper limbs in calcinosis associated with Sjögren’s syndrome, with two case reports of massive calcinosis affecting the elbows, knees and thighs. Although several predictive factors have been suggested for the development of calcinosis in systemic sclerosis (including CREST syndrome, anticentromere AK, concomitant arthritis), dermatomyositis (including prolonged disease duration, poor disease control, presence of Gottron’s papules), and systemic lupus erythematosus (including concomitant lupus nephritis, poor disease control), there are insufficient data for Sjögren’s syndrome.
Calcinosis cutis is difficult to treat, according to Dr. Akhila and colleagues. Therefore, surgical extirpation may be beneficial in the treatment of single or large lesions. However, recurrences and complications can occur, including delayed wound healing and infection. Calcinosis must be recognized as a rare manifestation of Sjögren’s syndrome. Further studies are needed to understand the prevalence, pattern and progression of this debilitating disease, the authors conclude. There is also a need to understand the pathophysiology in order to develop more targeted and effective therapies.
Literature:
- Akhila APV, et al: A Case of Calcinosis Cutis in a Patient With Sjögren’s Syndrome. AIM Clinical Cases 2024; 3: e231411; doi: 10.7326/aimcc.2023.1411.
InFo RHEUMATOLOGIE 2024; 6(2): 19
Cover picture: Milorad Dimic MD, wikimedia









