
Acoustic neuroma (schwannoma, neurilemmoma) is one of the most common benign tumors (WHO grade I) of the cranial nerves. The name has become established in the German-speaking world for tumor involvement of the vestibulocochlear nerve . Besides the neurinoma of the VIII. These space-occupying lesions also occur in the trigeminal and facial nerves, but to a significantly lesser extent.
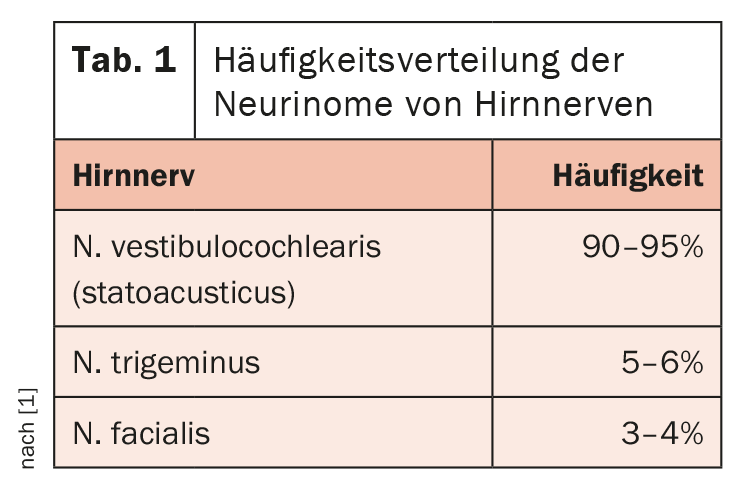
The frequency distribution of neurinomas of cranial nerves can be found in Table 1. Acoustic neuroma (AKN) is found unilaterally in most cases, but often bilaterally as a directional finding in neurofibromatosis type 2. Very rare are neurinomas of the motor cranial nerves such as oculomotor, trochlear or abducens nerve. The AKN occurs frequently in the 5. and 6th decade of life, somewhat more frequently in women. Children are affected only in the context of neurofibromatosis 2.
In the strict sense, AKN is not a brain tumor, but a benign mass of the peripheral nervous system [3]. They account for 8% of all intracranial tumors. With usually quite slow growth, the symptomatology appears very late. If the tumors remain small, symptoms of dizziness and hearing loss may not occur. If a slowly increasing hearing loss is noticeable, a hearing test may indicate the change. Typical is a deterioration of the high-frequency range (birdsong perceptible reduced). However, a sudden onset of hearing loss is also possible. Then, a very small intracochlear schwannoma should also be considered [5].
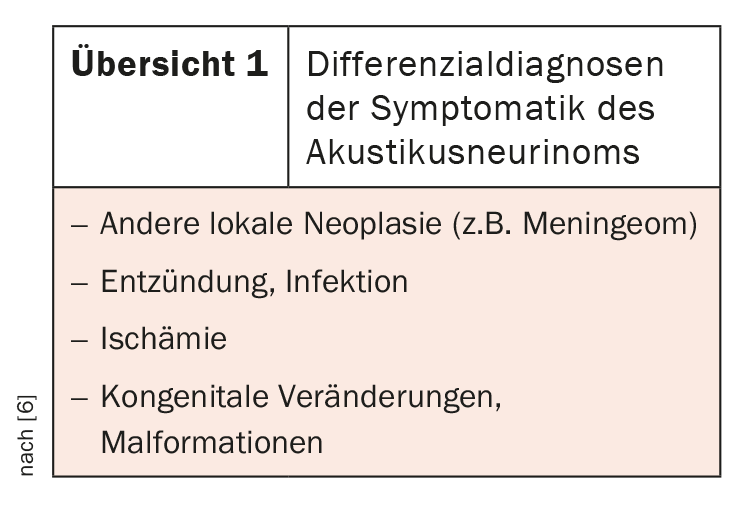
AKN can also be a possible cause of tinnitus, as well as cause spinning and swaying vertigo accompanied by nausea and/or nystagmus. In very rare cases, large neurinomas may cause cerebrospinal fluid circulation disturbance with pressure increase with headache, neck stiffness, nausea, vomiting, and visual disturbance. Subarachnoid hemorrhage caused by an AKN has been described [4]. The symptomatology requires a broad differential diagnosis (overview 1) with clinical, imaging and also laboratory chemical methods [6].
Therapeutically, surgical therapy can be performed for symptomatic neurinomas; increasingly, radiation therapy with Cyberknife is also used. X-rays of the skull no longer play a role in the diagnosis of acoustic neuroma. Computed tomographic examinations are not very suitable for detecting acoustic neuromas.
Imaging
The soft tissue contrast is lower than in MRI, and due to the considerable density differences between the petrous bone and the brain tissue of the cerebellopontine angle region locally in a small space, the so-called Hounsfield bar, a broad transverse stripe that is darkly imposing in the image, may limit the assessability [2]. Small AKNs may escape CT detection, especially in native diagnosis, and larger ones may be conspicuous by dilatation of the internal meatus acusticus.
Magnetic resonance imaging is the gold standard of acoustic neuroma imaging. Intravenous contrast administration shows a marked increase in signal, and often the 2 histologic forms (Antoni type A and B) can be differentiated by the regressive changes of type 2 [1]. The overall extent with extra- and intrameatal portions is readily assessable. If AKN has only an extrameatal portion (about 20% of cases), differentiation from meningioma may be problematic. Rarely, cystic neurinomas occur, which can be assigned to different types in terms of image morphology [7].
Case studies
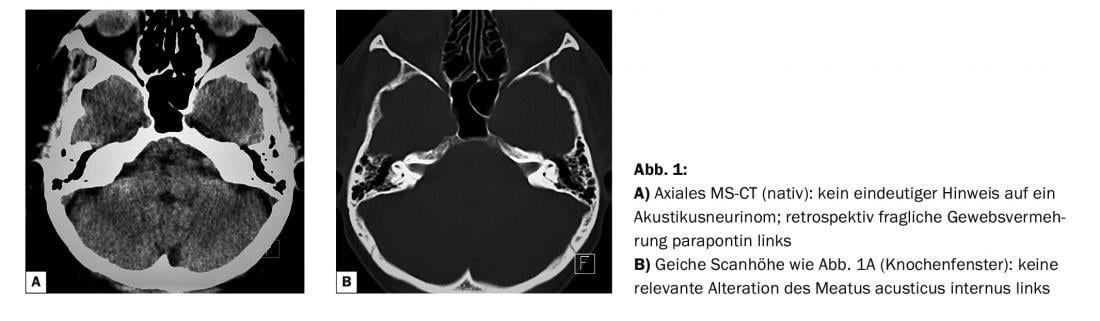
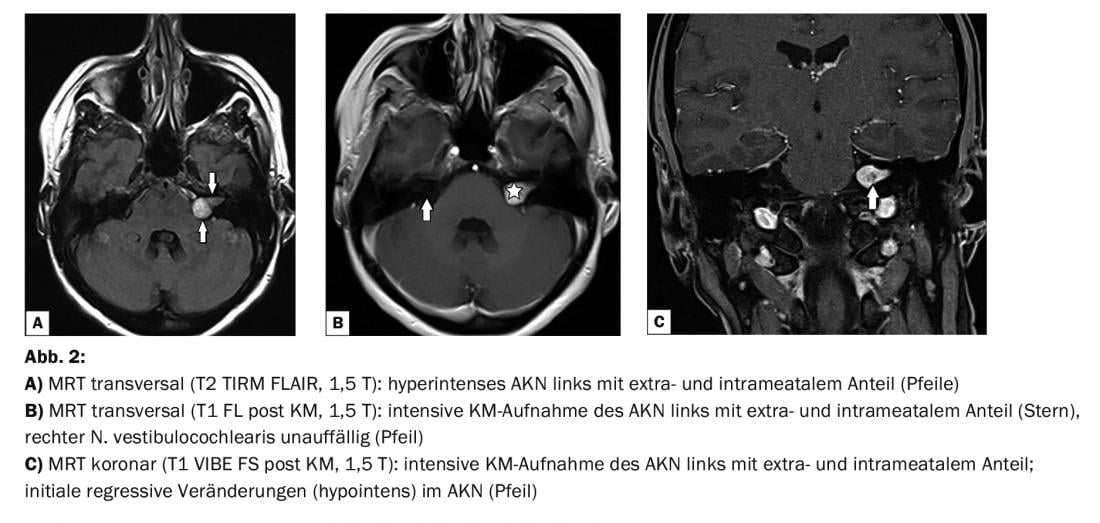
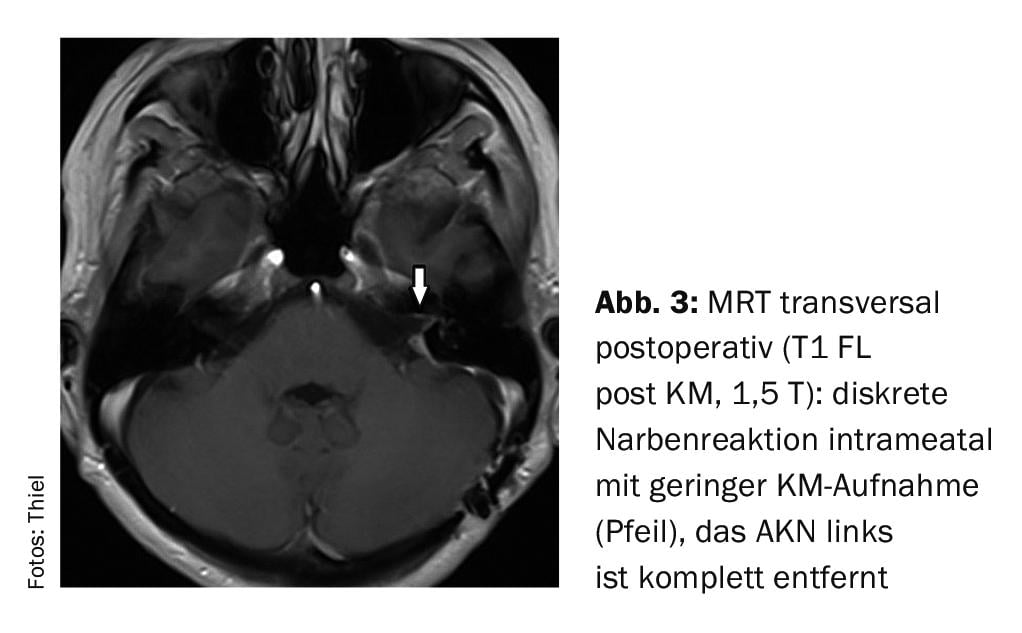
In case report 1, a 42-year-old female patient had been referred for native CT of the skull (Fig. 1A and B) to rule out exostosis. In the native scans, there were no abnormal findings in the brain. Two years later, dizziness and hearing loss occurred on the left side, which should be clarified by MR tomography. An acoustic neuroma with extra- and intrameatal portions (Fig. 2A to C) was diagnosed and surgically removed. Postoperative control (Fig. 3) was able to exclude residual or recurrent tumor 4 months after surgery with little intrameatal scarring.
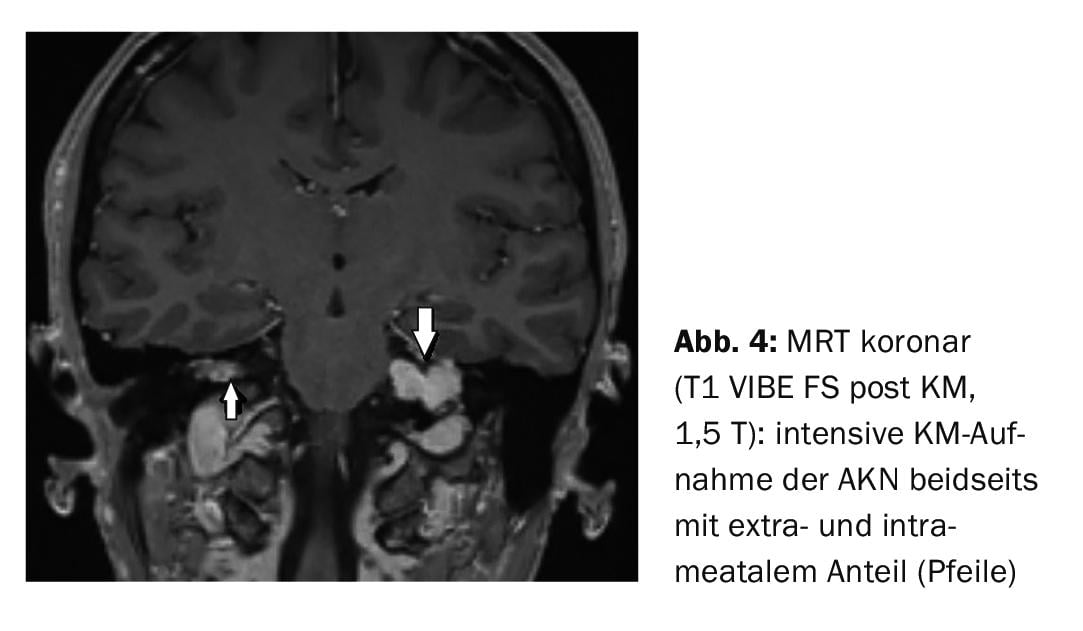
Case report 2 demonstrates bilateral acoustic neuroma in a 41-year-old female patient with neurofibromatosis. Both neurinomas are extra- and intrameatal in extent, the left one being larger than the right one (Fig. 4).
Take-Home Messages
- Neurinomas are benign tumors of the peripheral nerves.
- Acoustic neuroma is the most common benign intracranial space neoplasm.
- Schwannoma may be clinically silent, but often causes dizziness, hearing loss, or hearing loss.
- It usually occurs unilaterally; bilateral findings are possible in neurofibromatosis type 2.
- In diagnostic imaging, MRI with intravenous contrast agent is the standard procedure.
Literature:
- Uhlenbrock D, Forsting M: MRI and MRA of the head. 2nd, completely revised and expanded edition. Georg Thieme Verlag Stuttgart, New York 2007; 89-91.
- Sartor K: Neuroradiology. 2nd, completely revised and expanded edition. Georg Thieme Verlag Stuttgart, New York 2001; 106.
- Schwarz R: Acoustic neuroma. www.netdoktor.de.
- Fine R, Williams B, Dowling J: Acoustic neuroma causing subarachnoid haemorrhage. Med J Aust 1977 Jan 29; 1(5): 137-139.
- Miller ME, Moriarty JM, Linetsky M, et al: Intracochlear schwannoma presenting as diffuse cochlear enhancement: diagnostic challanges of rare cause of deafness. Ir J Med Sci 2012; 181(1): 131-134.
- Spickler EM, Govila L: The vestibulocochlear nerve. Semin Ultrasound CT MR 2002; 23(3): 218-237.
- Kameyama S, Tanaka R, Kawaguchi T, et al: Cystic acoustic neurinomas: studies of 14 cases. Acta Neurochir (Vienna) 1996; 138(6): 695-699.
InFo PAIN & GERIATry 2021; 3(2): 34-35.
InFo NEUROLOGY & PSYCHIATRY 2022; 20(1): 22-23.









