If geriatricians wanted to explain their focus to other physicians, they would quickly arrive at geriatric assessment (GA) as a special identifier. In order to exchange experiences in the use of assessment instruments and to initiate a process of continuous optimization of GA, the author of this article founded the “Assessment Working Group” anchored in the German Geriatrics Society in 2012. With the participation of people from this working group, the S1 guideline “Geriatric Assessment Level 2” could be published in 2019, which will be transformed into a “Living Guideline” with annual updates under the care of the Assessment WG in 2021.
If geriatricians wanted to explain their focus to other physicians, they would quickly arrive at geriatric assessment (GA) as a special identifier. Marjorie Warren called for a GA to be conducted 80 years ago before deciding whether to move to a long-term care facility. Bernhard Stuck’s meta-analysis published in 1993 [1] also set a milestone in the history of GA and underpinned the need to follow up the findings generated by means of GA with therapeutic action, if this is to bear the desired fruit. In the same year, he sat down with fifteen geriatricians and a sociologist from German-speaking countries, and two years later this “Geriatric Assessment Working Group” (AGAST) published for the first time a compilation of ten instruments under the title “Geriatric Basic Assessment – Guidelines for Action in Practice”, the regular use of which was to lay “a good foundation and starting point for further developments” [2]. In 2011, the repertoire of available tools had already expanded to such an extent that the brochure published by the Austrian Society for Gerontology and Geriatrics was able to present 31 instruments. In order to exchange experiences in the use of assessment instruments and to initiate a process of ongoing optimization of GA, the author of this article founded the “Assessment Working Group” in 2012, which is anchored in the German Geriatrics Society and now includes members of various professions of the geriatric team and their professional societies from the D-A-CH region. With significant participation of persons from this working group, the S1 guideline “Geriatric Assessment Level 2” could be published in 2019, which was transferred into a “Living Guideline” with annual updates under the care of the Assessment WG in 2021 [3].
Classification of the assessment
Assessment is a diagnostic process that usually takes place as a collaboration of different professions, in which, in addition to tests with and without performance, anamnestic data, previous findings and current clinical examination findings are also taken into account – therefore the colloquial titling of assessment instruments in the narrower sense as “assessments” is incorrect, they merely represent particularly characteristic elements. The attending physician is where the information comes together, and he or she moderates the activity of the team conducting the assessment so that no piece of the puzzle is missing and the overall picture can be correctly assembled together.
The S1 guideline follows the AGAST classification of GA into three levels: Level 1 assessment corresponds to a screening to find geriatric patients (the AGAST called this a modified screening according to Lachs), and level 3 more specific diagnostics that are only required in individual cases for more in-depth clarification of specific problems found. The broad field of GA is determined by the level 2 assessment, the “basic assessment”. For the first time, the S1 Guideline differentiates this into two sublevels: When the patient enters stage 2a, he or she has already been classified as “geriatric” – now as many of the situationally relevant dimensions (domains) as possible are examined to determine whether there is evidence of a need for treatment. If such a suspicion arises on the basis of the instruments used or other anamnestic or clinical indications (!), the assessment should be supplemented to level 2b with regard to this dimension. Only instruments that also provide indications of the degree of impairment and can thus be used to map the course – an increase in severity as the underlying disease progresses or the constellation of contextual factors becomes less favorable, but also a reduction in severity, e.g., as a result of successful therapy – are suitable for this sublevel.
Structure of the S1 Guideline
The 2021 updated version of the S1 guideline is also a rather short long version despite its 103 pages, since a large part of the lines is reserved for the 55 standardized tables in boxed format characterizing the assessment instruments. The order in which tools used for the same dimension are mentioned is based on the factor that also often tips the scales in clinical practice when deciding which of the competing tests will ultimately be introduced: time requirements. Thus, for cognition, 15 procedures of one to twenty minutes duration are mentioned. Information is also provided on the learning effort required by examiners, the professions that commonly use this test, the focused severity level, quality criteria, limitations, research needs, and literature references. A special feature of the guideline with regard to the naming of cut-off values is that the polarity is also clearly indicated with the cut-off (e.g., “cut-off 9/<9” means that 9 is still assessed as inconspicuous and below 9 as conspicuous). The boxes are preceded by a text regarding each of the dimensions, which relates the different tools to each other and should thus facilitate the selection in the search for the most suitable tool. A conscious decision has been made not to rank the quality of the instruments: Unsuitable instruments or those that are generally inferior to another instrument available in German are not listed; there cannot be a generally best instrument, since suitability in individual cases is also determined by comorbidities.
The dimensions
Without geriatric syndromes, an elderly person would not be a geriatric patient. Choosing as dimensions to be considered those to which the geriatric syndromes belong is an obvious step.
In the first update of the S1 guideline, reference is made to the gap still to be closed with regard to the assessment of communication skills, in which hearing and vision are included as parts of the sensory system that are affected more frequently in typical old age – and deficits in these can also impair independence and quality of life outside of interpersonal contacts. A new addition to the update is already the dimension of continence, whereby reference is made to the already existing S2e guideline “Urinary incontinence in geriatric patients” [4].
For nutrition assessment, the guideline cites the Mini Nutritional Assessment (MNA-SF) short form, the Malnutrition Screening Tool (MST), and the Nutritional Risk Screening (NRS). Furthermore, reference is made to the link to the ESPEN guideline “Clinical Nutrition and Hydration in Geriatrics” [5]. Closely related to the issue of malnutrition is the problem area of dysphagia. To elicit suspicious symptoms, the guideline lists the Standardized Swallowing Assessment (SSA) and Daniels’ predictors of aspiration. A separate subchapter is devoted to sleep and the Essen Questionnaire Age and Sleepiness (EFAS) [6] is presented for the standardized observation of daytime sleepiness in geriatric patients.
The Substance Abuse/Addiction subsection presents the CAGE Questionnaire, the Alcohol Use Disorder Identification Test-Consumption (AUDIT-C), and the Short Michigan Alcoholism Screening Test Geriatric Version (SMAST-G) for the assessment of alcohol dependence, and the Benzo Check for problematic benzodiazepine use.
Self-help capability
In the area of basic activities of daily living (B-)ADL, the ten-item Barthel index , published by Mahoney and Barthel as early as 1965, continues to play the undisputed leading role. By no means should it be assumed that an elderly person can only be a geriatric patient if the score drops. The operationalization according to the Barthel plus, which is based on the Hamburg Manual for the Barthel Index, therefore distinguishes at item level a sublevel with independent performance under impairment.
The early rehabilitation Barthel index introduced by Schönle in 1995 can assume values below zero by adding minus points for complex monitoring measures, e.g., tracheostoma. The Functional Independence Measure (FIM) published by Keith in 1987 could not establish itself in German-speaking countries despite theoretical advantages (seven-level scaling, inclusion of cognition).
In most cases, several of the instrumental abilities (IADLs) compiled by Lawton and Brody in 1969 are impaired much earlier than the ADLs listed in the Barthel Index, including the use of public transportation. No norm values are defined for the score across all eight three- to five-level formulated activities. Deviating from the original scoring system (0 or 1 point per item), several more differentiated scoring systems exist, the best known probably being the one introduced in St. Gallen. The increasingly important role of digital communication should prompt consideration of a modification that integrates it into the four-level item of ability to use the telephone – or to include a more up-to-date assessment tool in the guideline in the future. Performance on the money counting test introduced by Nicholas in 1995 is influenced by cognition, visual acuity, and fine motor skills. A conspicuous result raises doubts not only about the ability to deal practically with money, but also, for example, with medication schedules.
Mobility/motor skills
The Parker Mobility Score [7] (referred to as “A New Mobility Score…” in its initial publication in 1993, which was not intended to be a permanent name according to consultation with the first author) represents a minimal variant in the history of mobility with additional scoring. The question “What was it like before?” arises in particular when mobility has deteriorated significantly, e.g. due to a hip fracture. It is obvious that the therapy goal can hardly ever be set higher than it corresponds to the status before the acute event. The score also predicts mortality risk.
Podsiadlo and Richardson selected for the Timed Up & Go (TUG) described in 1991 those basic elements of mobility necessary to move independently at the room level. The normal value of less than ten seconds is only achieved by patients who have no major difficulties in walking speed (2 × 3 m) as well as in turning around (after 3 m and before sitting down) and in standing up/sitting down. According to the current European guideline [8], a time requirement of at least 20 seconds indicates a high degree of severity in the presence of sarcopenia. Most frequently, patients fail to stand up; about half of acute geriatric hospital patients cannot overcome this hurdle despite the possibility of using armrests or walking aids to support themselves.
If the TUG is mastered, the supplementary examination of the result as a TUG Dual Task under distraction by a cognitive task (e.g., the task to name as many different animal species as possible or to solve arithmetic problems) provides valuable information about gait safety under everyday conditions as well as about cognitive deficits. Less frequently, an additional motor task (holding a cup, turning the head) is used for this purpose.
Repeated standing up and sitting down without supporting the arms is the technically simplest method of obtaining conclusions about the strength of the muscles involved via the speed as lifting performance of portions of one’s own body weight. The 30 s Chair Stand Test lasts exactly as long as its name suggests – then the number of stand-up maneuvers is noted (e.g., 10×/30 s). In contrast, in the Five Chair Rise Test, the number of stand-up attempts is fixed. If the task is not yet completed when the time limit of one minute is reached, noting the result serves to reduce the “floor effect”, because even starting from e.g. 3×/60 s, a further deterioration to 2, 1 or 0 successful stand-up attempts is possible – but also an improvement to 4× before the task can be completely fulfilled. A five chair rise test of more than 15 seconds is considered an indication of possible sarcopenia according to the current European guideline [8].
Tests of walking speed are also defined either by duration or by the amount of what is accomplished – in this case, distance. The latter is the rule for short tests that can also be performed in the office or home (e.g., the 4-meter walk test). One meter of acceleration and braking distance should be available in front of and behind the test track, respectively. The longer the walking test, the more the cardiopulmonary performance and the blood flow to the leg muscles are included in the result – basically, even in intermittent claudication, the total distance covered within six minutes, for example, is more relevant to everyday life than the (speed-dependent) distance to the first standing stop. In the presence of sarcopenia, values from 0.8 m/s correspond to a high degree of severity [8].
The 15 items of the de Morton Mobility Index (DEMMI) [9,10] cover a wide range of severity of mobility impairment (from “bridge building” in the supine position to tandem standing with eyes closed and jumping) with, however, a maximum three-level rating of the respective performance. As a result, floor and ceiling effects are small, but little differentiation below independent walking ability is expected.
While the Berg Balance Scale and the Tinetti test (=POMA I and II) are used less and less in geriatrics, the Short Physical Performance Battery (SPPB) has become the currently best-known combination of subtests of mobility, not least because of the extensive international literature [11]. Sarcopenia is considered severe if a total of less than 9 of the maximum 12 points are achieved in the total of 5 tasks (3× balance, five chair rise test, walking test) [8].
Fear of falling can occur even in the absence of physical trauma and can increase gait insecurity precisely via avoidance behaviors. Concerns about falling can be assessed in a standardized way using the Falls Efficacy Scale-International or its short form (FES-I, Short FES-I) [12,13].

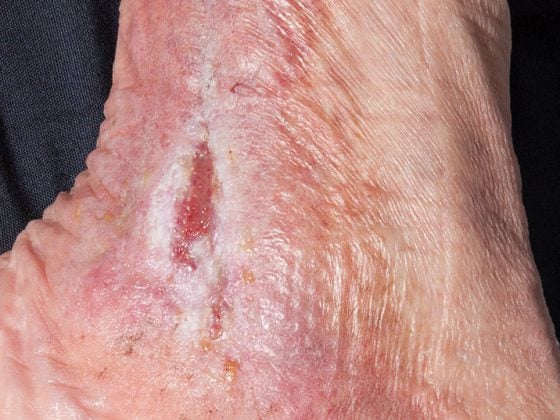
The measurement of hand force (gripping force, Fig. 1) is often used in the literature as a correlate of the strength level of the other body regions as well, which would be more technically complex to assess. Sarcopenia is suspected in women who have less than 16 and men who have less than 27 “kg” (the most commonly reported unit, although reluctant to any physicist) of hand strength [8]. The function of the hand in many activities is determined less by hand strength than by fine motor skills. The 20-Cents Test (20-Coins Test, 20-C-T, Fig. 2) [14] records the speed at which 20 coins (validated on European and U.S. 1-cent coins) are transported individually from a sheet of drawing pad paper into a collecting vessel. With more than 40 seconds of time required for one hand, impairment of activities of daily living is to be expected.

Cognition
The Mini Mental State Examination (MMSE) [15] is in many countries the test whose result is expected as a reference value in the communication e.g. with cost units, despite the difficult application due to late licensing and clear weaknesses both in the early detection and in the differentiation of strongly advanced dementias. There are adaptations to severely visually impaired people [16].
Callahan developed the Six-Item Screener (SIS) [17] from the items of the Mini Mental State Examination that are usually the earliest to respond in Alzheimer’s disease, in order to have an instrument that can also be used by telephone when seeking individuals who are cognitively capable of study participation. The validation of the German translation [18] confirmed the suitability of the one-minute, material-free test as a level 2a assessment instrument (i.e., if there are abnormalities in the test, anamnestic or clinical, another test should follow).
Although clock tests (Fig. 3) , like the SIS, are not suitable for describing dementia in isolation, they are interesting combination partners due to the recording of other aspects of cognition and strike significantly earlier in most forms of dementia, also in comparison with the MMSE. Despite slightly different tasks and significantly different scoring systems, the watch tests exhibit similar quality criteria. In Germany, the watch test according to Shulman, as modified in 1993, is currently favored as the easiest to learn; in addition, the guideline mentions the tests according to Sunderland 1989 and Watson 1993. In Switzerland, the Thalmann 2002 watch test is also well known.

Mini-Cog [19] and “Fast Clock Triples ” [20] combine a clock test with coarser scoring and the task of repeating three terms after distraction. The Brief Alzheimer Screen [21] is suitable for the early detection of Alzheimer’s disease – regardless of the visual acuity and fine motor skills of the person examined. However, a validated German translation of the test is still missing. The Bamberg Dementia Screening Test [22,23] also does not require any material and offers the possibility to terminate the test if the result is “positive” after only two tasks and to proceed directly to neuropsychological testing (level 3 of the assessment). The use of tapping sequences as tasks is interesting.
The Montreal Cognitive Assessment (MoCA) [24] is experiencing a resurgence internationally due to higher sensitivity in early detection of dementia development compared to the MMSE, as well as translations available in many languages and additional adaptations (e.g., the HI-MoCA [25]). The Memory Clinic Basel provides an online calculation with age, gender, and education adaptations [26]. Since 2019, downloading the test requires registration on the official MoCA website, and depending on the application, also the completion of a training program with certification.
Both the DemTect [27] and the Test for Early Detection of Dementia with Depression Delineation (TFDD) [28] are dedicated to detecting even mild cognitive impairment, and both were developed in German. For the DemTect, (stricter) scoring is also available for people under 60. The TFDD includes the watch test to Sunderland. A special feature is the numerical rating of depressiveness from the perspective of both the patient and the examiner, which is added to a score (0-10 points each, need for clarification if more than 8 points).
The Severe Mini Mental State Examination (SMMSE) [29,30] spares many patients beyond the middle stage of dementia the frustration often leading to test discontinuation due to overwhelm when further monitoring of progress is indicated. Strotzka et al. published a German translation validated in Vienna in 2005.
The Global Deterioration Scale [31] is used primarily for advanced Alzheimer’s dementia. It is the only one of the cognition instruments mentioned in the guideline that does not involve a testing situation for the patient. External assessment of remaining abilities or symptoms caused by dementia development requires in-depth knowledge of the patient and is usually based on information provided by the primary caregiver. For the assessment of delirious states, the guideline cites the Nursing Delirium Screening Scale (NU-DESC), the Delirium Observation Screening Scale (DOSS ), and the Confusion Assessment Method (CAM).
Depressiveness
The guideline follows the recommendations of the AGAST to focus at least on depressiveness from the diverse subdimensions of emotionality. A realistic assessment cannot be expected in the exceptional situation of the day of admission to inpatient hospital care; especially for the longer instruments, the patient and examiner should allow themselves a somewhat calmer atmosphere and time for reflection.
The Geriatric Depression Scale (GDS) [32] recommended by the AGAST in its shortened version from 30 to 15 items will probably continue to be the most frequently used; in addition, various even shorter versions exist, some with different item combinations. Here, care must be taken to strictly adjust the cut-off so as not to reduce sensitivity.
The 2-question test according to Whooley [33] achieves astonishing sensitivity with the questions “In the past month, have you often felt down, sadly depressed, or hopeless?” and “In the past month, have you had significantly less pleasure and joy in doing things you usually enjoy?” (in the initial publication, outpatient 96%; data from inpatient acute geriatrics will be published in 2022 by the author of this article). This makes the test suitable for a level 2a assessment – if depression is suspected, the assessment must be continued.
The WHO 5 well-being index, published in 1998. stands out from the other survey instruments in that all five items are positively worded (e.g., “In the last two weeks, I have been happy and in a good mood – all the time / most of the time / a little more than half the time / a little less than half the time / now and then / at no time”) with the highest score for the longest duration of well-being, i.e., “all the time,” and zero points for “at no time.” This allows milder depression to be recorded. The six-level scaling maps changes in mood.
Also, the depression section of the Patient Health Questionnaire (PHQ-9) [34] should indicate how often each of the 9 depressive symptoms had occurred in the previous two weeks. A four-level choice is given. The last item directly addresses death wish and the desire to “inflict suffering”.
The Depression in Aging Scale [35] gets by with 10 statements, which, as in the GDS, are collected as yes/no responses. The sentence structure is much simpler compared to the GDS. In old age, anxiety and depression often contribute simultaneously to a loss of quality of life. The two subscales of the Hospital Anxiety and Depression Scale (HADS) [36] each contain seven items rated on four levels.
The only third-party assessment scale listed in the guideline is the Montgomery Asberg Depression Rating Scale (MADRS) [37,38]. The seven-point rating of 10 items provides room for changes in the score according to the severity of depression. Information from family members and observations by other members of the geriatric team can be included in the assessment, as can the patient’s expressions and facial expressions. This offers advantages especially for psychologically stressed and cognitively impaired patients.
Pain
The subchapter of the guideline dealing with pain assessment was designed in cooperation with the working group “Pain and Aging” of the German Pain Society. In terms of a level 2a assessment for patients who can be assessed, it is recommended to first ask about current pain, then whether there has been pain in the past two weeks, and if the answer is yes, whether the patient expects it to occur again in the next two weeks. Current or anticipated pain should be assumed to require therapy or clarification. Any waiver of this requirement – e.g. at the express request of the patient – must be documented together with the reasons for the waiver.
The level 2b pain assessment includes the following aspects:
- the assessment of pain intensity, where a numerical scale (0-10 or as a percentage of the maximum imaginable pain) is usually better understood than a visual scale, but a verbal rank scale with fixed terms is even easier (to allow comparability when assessed by different examiners as well as during the course)
- Documentation of pain localization (in words or by drawing in a schematic diagram).
- Describe the character of the pain (preferably exactly as the patient formulates it, if necessary offer terms from a pre-formulated list)
- the “pain schedule” (“How long have you known this pain? How often does it occur and for how long?”)
- the pain triggers (triggered by certain movements/positions/rest?)
- the pain relievers (positive therapy experiences medicamentous and non-medicamentous, self-help, also beddings, cold/warmth, anointings)
External assessment scales for use with patients who cannot verbally express possible pain are to be assigned to level 2b of the assessment. The guideline cites the Scale for the Assessment of Pain in Dementia (BESD scale) [39] and the Observational Instrument for Pain Assessment in the Elderly with Severe Dementia (BISAD scale) [40].
Take-Home Messages
- The geriatric assessment is a diagnostic process which, in addition to the application of assessment instruments, also includes anamnesis and clinical examination and integrates already existing findings.
- Geriatric assessment is usually performed interprofessionally as a team effort, with the attending physician responsible for designing it to meet the patient’s needs as closely as possible.
- The decision on which dimensions to focus on in the assessment is followed by the selection of the most appropriate assessment instruments in the individual case – the patient’s comorbidities play a crucial role.
- Efficient assessment addresses the dimensions at different levels of clarification (2a: no indication/indication of need for therapy, 2b: recording of severity) and combines instruments without and with performance.
Literature:
- Stuck AE, Siu AL, Wieland GD: Comprehensive geriatric assessment. A meta-analysis of controlled trials. Lancet 1993; 342: 1032-1036.
- Geriatric Assessment Working Group (AGAST). Geriatric baseline assessment. Guidance for practice; Geriatrics Practice Series. MMV Medizin Verlag Munich 1995.
- Krupp S. for the AG Assessment of the Deutsche Gesellschaft für Geriatrie e.V.S1-Leitlinie Geriatrisches Assessment der Stufe 2, Living Guideline, Version 15.10.2021, AWMF-Register-Nr. 084-002LG.
- Wiedemann A, for the Incontinence Working Group of the German Geriatric Society: S2e Guideline Urinary Incontinence in Geriatric Patients, Diagnosis and Therapy. AWMF Reg. no. 084 001Long version 2019; www.awmf.org/uploads/tx_szleitlinien/084-001l_S2e_Harninkontinenz_geriatrische_Patienten_Diagnostik Therapy_2019-01.pdf (accessed 10 Oct 2021).
- Volkert D: Current ESPEN guideline Clinical nutrition and hydration in geriatrics. Dtsch Med Wochenschr 2020; 145(18): 1306-1314; doi: 10.1055/a-0986-2892.
- Frohnhofen H, Bibl M, Nickel B, Popp R: The Essen Questionnaire on Aging and Sleepiness (EFAS) – a new assessment tool for measuring daytime sleepiness in the elderly. Euro J Ger 2010; 12: 84-90.
- Parker MJ, Palmer CR: A new mobility score for predicting mortality after hip fracture. J Bone Joint Surg Br 1993; 75: 797-798. German in: Krupp S.: Geriatric assessment. In: Willkomm M (ed.) Praktische Geriatrie. 2nd ed. Georg Thieme Verlag 2017, Stuttgart, p.41.
- Cruz Jentoft AJ, Bahat G, Bauer J, et al: Sarcopenia: revised 14 European sensus on definition and diagnosis. Ageing 2019; 48: 16-31; doi: 10.1093/ageing/afy169.
- De Morton NA, Jones CT, Keating JL: The de Morton Mobility Index (DEMMI): An essential health index for an aging world. Health Qual Life Outcomes 2008; 6: 63.
- Braun T, Schulz RJ, Reinke J, et al: Reliability and validity of the German translation of the de Morton Mobility Index (DEMMI) performed by physiotherapists in patients admitted to a sub-acute inpatient geriatric rehabilitation clinic. BMC Geriatr 2015; 15: 58.
- Guralnik JM, Simonsick EM, Ferrucci L, et al: A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nurs-ing home admission. J Gerontol 1994; 49: M85-M94.
- Kempen GI, Todd CJ, Van Haastregt JC, et al: Cross-cultural validation of the Falls Efficacy Scale International (FES-I) in older people: results from Germany, the Netherlands and the UK were satisfactory. Disabil Rehabil 2007; 29: 155-162.
- Kempen GI, Yardley L, van Haastregt JC, et al: The Short FES-I: a shortened version of the falls efficacy scale-international to assess fear of falling. Ageing 2008; 37: 45-50.
- Krupp S, Kasper J, Balck F, et al: “Timed up and go” for the fingers in the form of the 20 cents test. Psychometric quality criteria of a simple fine motor performance test. Z Gerontol Geriat 2015; 48: 121-127.
- Folstein MF, Folstein SE, McHugh PR: “Mini-Mental State” – A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975; 12: 189-198.
- Reischies FM, Geiselmann B: Age-related cognitive decline and vision impairment affecting the detection of dementia syndrome in old age. Br J Psychiatry 1997; 171: 449-451.
- Callahan CM, Unverzagt FW, Hui SL, et al: Six-item screener to identify cognitive impairment among potential subjects for clinical research. Med Care 2002; 40: 771-781.
- Krupp S, Seebens A, Kasper J, et al: Validation of the German version of the Six-Item Screener. Cognitive short test with broad application possibilities. Z Gerontol Geriat 2018; 51: 275-281.
- Borson S, Scanlan JM, Chen P, Ganguli M.: The Mini-Cog as a screen for dementia: Validation in a population-based sample. JAGS 2003; 51: 1451-1454.
- Strotzka S, Psota G, Sepandj A: Clock testing in dementia diagnostics – In search of lost time. Psychopraxis 2003; 04/03: 16-24.
- Mendiondo MS, Ashford JW, Kryscio RJ, Schmitt FA: Designing a Brief Alzheimer Screen (BAS). J Alzheimers Dis 2003; 5: 391-398.
- Trapp W, Weisenberger B, Düclos D, et al: The Bamberg Dementia Screening Test (BDST) – first evidence regarding the diagnostic usability of a “true bedside” test for geriatric inpatients. Z Neuropsychol 2015; 26: 161-170.
- Trapp W, Röder S, Heid A, et al: Sensitivity and specificity of the Bamberg Dementia Screening Test’s (BDST) full and short versions: brief screening instruments for geriatric patients that are suit-able for infectious environments. BMC Med 2021; 19: 65.
- Nasreddine ZS, Phillips NA, Bedirian V, et al: The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005; 53: 695-699.
- Lin VY, Chung J, Callahan BL, et al: Development of cognitive screening test for the severely hearing impaired: Hearing-impaired MoCA. Laryngoscope 2017; (127) Suppl 1: S4-S11.
- www.mocatest.ch/de/standardwerte/standardwerte-online-berechnen (accessed Dec. 20, 2021).
- Kalbe E, Brand M, Kessler J, Calabrese P: The DemTect in clinical application. Journal of Gerontopsychology & Psychiatry 2005; 18: 121-130.
- Ihl R, Grass-Kapanke B, Lahrem P, et al: Development and validation of a test for early detection of dementia with depression delineation (TFDD). Fortschr Neurol Psychiatr 2000; 68: 413-422.
- Harrell LE, Marson D, Chatterjee A, et al: The Severe Mini-Mental State Examination: a new neuropsychologic instrument for bedside assessment of severely impaired patients with Alzheimer disease. Alz Dis Assoc Dis 2000; 14: 168-175.
- Strotzka S, Sepandj A, Psota G: Severe Mini Mental State Examination – Neuropsychology for people with severe dementia. Psychopraxis 2005; 6: 10-15.
- Reisberg B, Ferris SH, de Leon MJ, Crook T: The global deterioration scale for assessment of primary degenerative disease. Am J Psychiatry 1982; 139: 1136-1139.
- Yesavage JA, Brink TL, Rose TL, et al: Development and validation of a geriatric depression screening scale. A preliminary report. J Psychiatr Res 1982; 17: 37-49.
- Whooley MA, Avins AL, Miranda J, et al: Case-finding instruments for depression. Two ques-tions are as good as many. J Gen Intern Med 1997; 12: 439-445.
- Spitzer RL, Kroenke K, Williams JB, et al: Validation and utility of a self-report version of PRIME-MD. The PHQ Primary Care Study. JAMA 1999; 282: 1737-1744.
- Heidenblut S, Zank S: Development of a new depression screening for use in geriatrics. The Depression in Aging Scale (DIA-S). Z Gerontol Geriatr 2010; 43: 170-176.
- Zigmond AS, Snaith RP: The hospital anxiety and depression scale. Acta Psychiatr Scand 1983; 67: 361-370.
- Montgomery SA, Åsberg M: A new depression scale designed to be sensitive to change. Br J Psychiatry 1979; 134: 382-389.
- Schmidtke A, Fleckenstein P, Moises W, Beckmann H.: Studies on the reliability and validity of a German version of the Montgomery-Åsberg Depression Rating Scale. Swiss Arch Neurol Psychiat 1988; 139: 51-65.
- Basler HD, Hüger D, Kunz R, et al: Assessment of pain in dementia (BESD). Pain 2006; 20: 519-526.
- Fischer T: Pain assessment in people with severe dementia. The Observation Instrument for Pain Assessment in the Elderly with Severe Dementia (BISAD). Bern 2012: Verlag Hans Huber.
HAUSARZT PRAXIS 2022; 17(6): 4-9