
In March 2019, the Federal Office of Public Health plans to publish the new vaccination schedule. Dr. Niederer-Loher from KS St. Gallen gave a first insight at the medical congress in Davos. This much in advance: the vaccination scheme becomes easier.
That is the message of Anita Niederer-Loher, MD, senior physician at the Clinic for Infectiology and Hospital Hygiene of the Cantonal Hospital of St. Gallen. The epidemiological situation has changed, which is why the 2018 vaccination recommendations still in effect (Table 1) are now being amended. These changes also contribute to simplification.
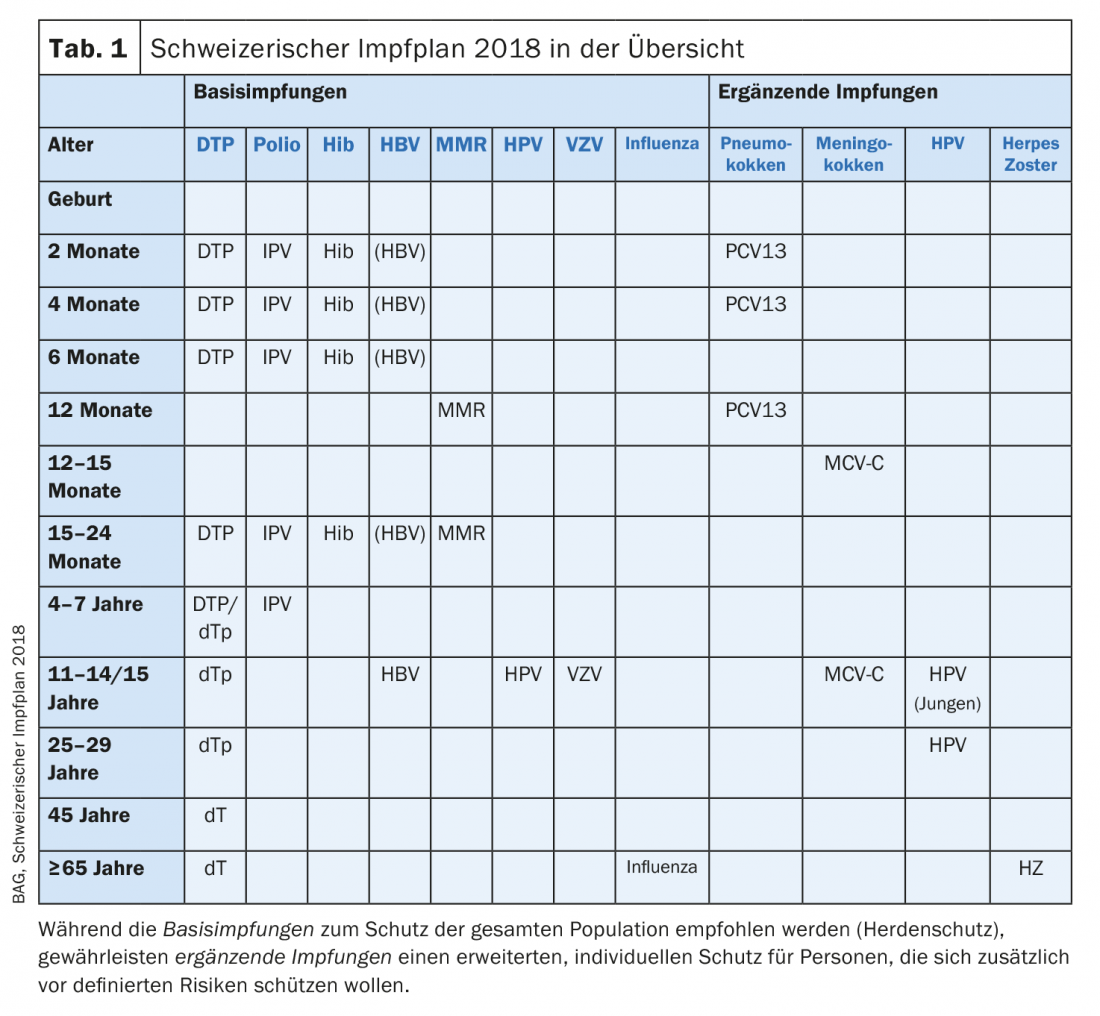
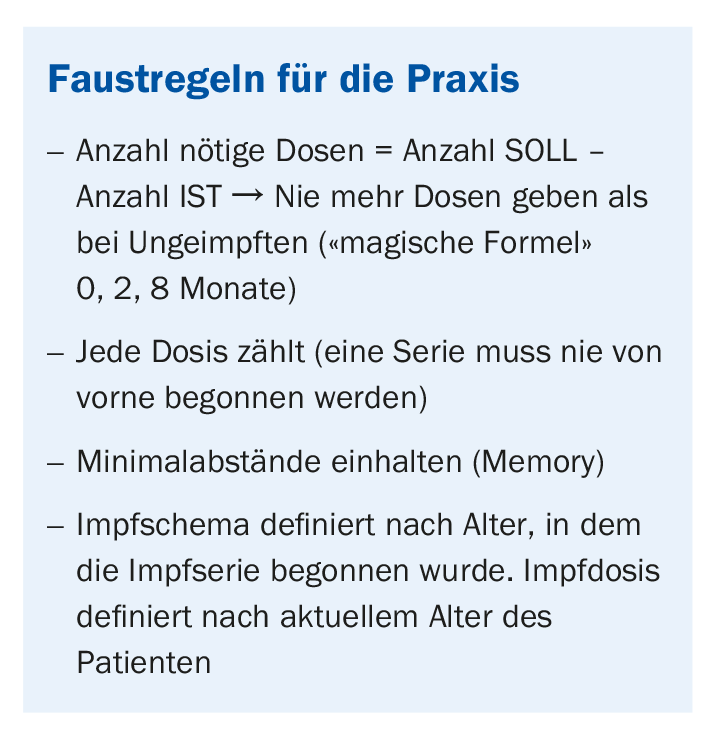
The vaccination scheme is still relatively complicated. In three tables, the 2018 Immunization Schedule provides information on catch-up vaccinations for incompletely vaccinated or unvaccinated individuals. Those who do not want to struggle through these numbers will soon be able to use the simple scheme that will apply from March 2019: The basic immunization formula “0, 2, 8 months”. This “magic formula” applies to most vaccinations. Those who have never been vaccinated receive the first vaccination at time 0, the second after two months, and the third eight months later.
Basically, every dose counts! This means that even if a vaccination was given decades ago, it does not have to be started all over again. It is important that the minimum distances between the cans are maintained so that the memory effect occurs. If a patient has received the first dose (0) but does not reappear for three years, he will receive the second dose (2) and six months later the third (8). Incidentally, there is no danger from “overvaccination,” as Dr. Niederer-Loher emphasizes.
What’s new?
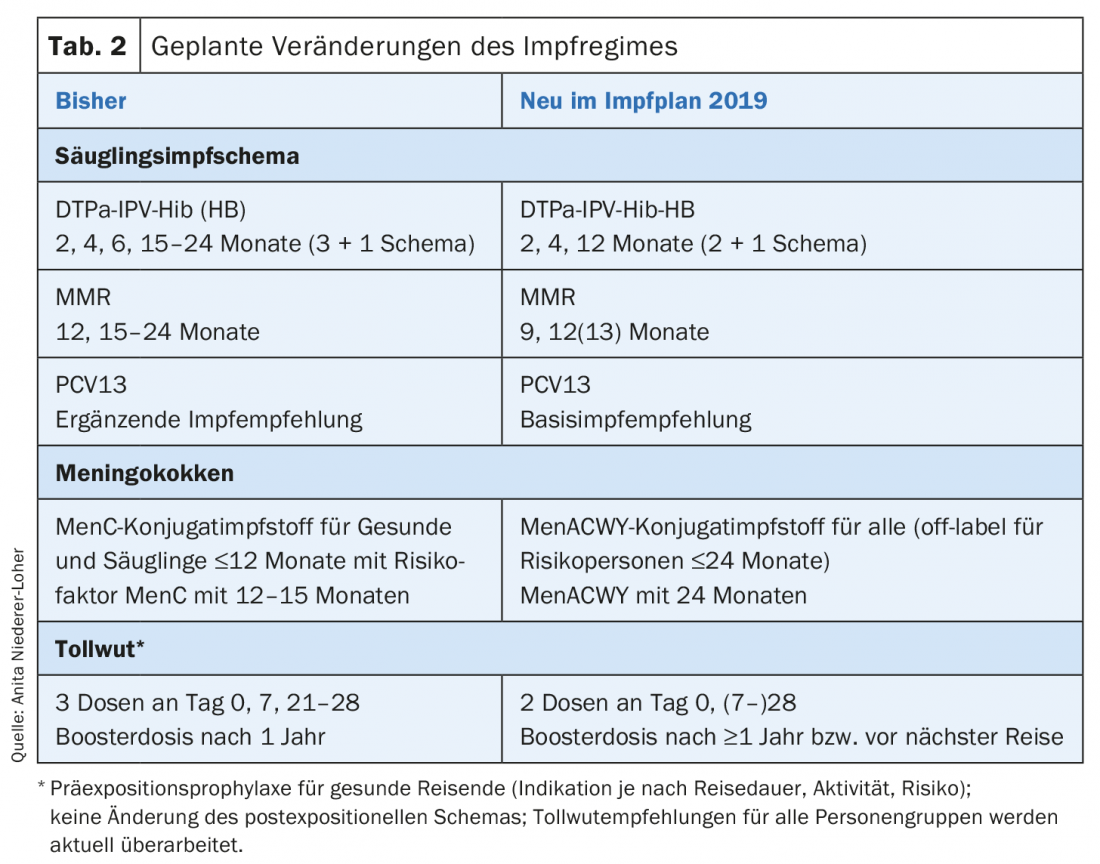
The current infant vaccination schedule is 3 + 1. Vaccinations are given in the first year of life at two, four, and six months of age and, after a memory phase, at 15-24 months of age. Good protection is guaranteed after about two doses. Therefore, to protect the infant, expectant mothers must already be vaccinated against pertussis: Many severe cases of pertussis occur in the first 2-3 months of life – too early for vaccination of the infant alone to prevent infection. Beginning in March, the new immunization schedule will put the infant immunization schedule 2 + 1 into effect. This is already practiced by many European countries, such as Denmark, Sweden, France and Austria. For Switzerland, this specifically means hexavalent vaccination at 2, 4 and 12 months. By reducing to 2 priming doses (and correspondingly lower antibody titers), booster administration occurs earlier than before at 12 months. In addition to DTPa, IPV and Hib, HB now also becomes an integral part of the scheme.
With regard to meningococci, MenC vaccination is being replaced by quadrivalent vaccination in infants, adolescents, and at-risk groups because cases with meningococci W and Y in particular have increased significantly. However, vaccination of infants is not done until 24 months of age.
For rabies, as of 2019, two doses can be administered pre-exposure, ideally on days 0 and 28; if the patient travels earlier, the timing of the second dose can be scheduled up to 7 days after administration of the first. A booster is still absolutely necessary (Tab. 2).
The misery with the vaccination refusers
An outbreak of measles at a Biel school is currently making headlines. In early February, the teaching staff learned that a student had contracted measles. Although authorities responded immediately and sent all unvaccinated children home for three weeks, 14 children contracted the highly contagious disease. This case once again fuels the media discussion about the fundamental question: Vaccination – yes or no?
Opponents argue, among other things, that vaccinations could result in complications, while infections are important experiences for the child’s development. Dr. Niederer-Loher disagrees. She pleads for consistent vaccination coverage with regard to measles and criticizes that Switzerland is lagging behind worldwide in this regard. While the rate in this country is 94%, Zimbabwe reaches 95% and Botswana even 97%. To achieve the WHO’s goal of measles eradication, a rate of 95% is needed. So there is still a lot to be done. The vaccination brochure “Vaccinate children?” provides doctors with a set of arguments for dealing with recalcitrant vaccination refusers. Yes! Why?”, which is available on the Infovac website (Swiss information platform for vaccination issues).
can be.
Determine and document vaccination status
For the initial evaluation of the vaccination status, Dr. Niederer-Loher recommends a routine procedure: “It is important that you get into the habit of doing things the same way every time. Look at each disease individually in your target-actual balance sheet. If you know what the patient needs, you can look at which vaccine has it all.” The dose is the difference between recommended vaccination status and actual vaccinations given in the patient.
>Tip: The vaccination card is also available as an electronic tool www.meineimpfungen.ch
Source: 58th Davos Medical Congress, February 7-9, 2019.
FAMILY PRACTICE 2019; 14(3): 37-39









